Changing places - but not that fine-tuned focus
From first lady of breast MRI to the Germany’s most influential woman in radiology – that’s one way to describe Professor Christiane Kuhl’s switch from being Vice-Chairman of the Department of Radiology and Vice President of the University of Bonn to become Chairman of the Department of Diagnostic and Interventional Radiology at the University Hospital Aachen (UKA).


Since taking on this leadership role in May 2010, the radiologist has been constantly scrutinised by the male top management in university radiology as well as by her critics around the issue of MRI for the early detection of breast cancer.
Asked how she feels about being a ‘centre of power’, Professor Kuhl answered calmly: ‘I believe that power and influence are more likely to give men a rush of happiness than women. The main reason for my decision to take the post at the UKA was the appeal of being able to develop radiology based on my own beliefs – and it shouldn’t be my own personal interests that are at the forefront here, but those of the patients. Human beings should be the centre of attention.’
The signs were particularly good for a new start in Aachen -- there were as many as 20 new chairman positions to be filled in different departments, e.g. abdominal and transplant surgery, orthopaedics, urology, neurosurgery, cardiology, oncology, nuclear medicine, and so forth. The result is an unusually young team of Department directors who meet ‘at eye level’ and share a common focus – oncology. This was an outstanding opportunity for Professor Kuhl to develop interventional radiology further, alongside her ‘hobby horse’ -- breast diagnostics. A personal dream, as ‘breast diagnostics as well as oncologic interventions mean that the radiologist assumes full clinical responsibility and takes active care for his or her own patients’.
There is also an element of personal triumph in being able to show her critics that the new director can offer more than just breast cancer diagnostics. As during her time at the university of Bonn, Prof. Kuhl now puts a particular focus on major liver interventions. Since her arrival, she has introduced SIRT, new TACE procedures and set new standards for oncologic interventions as a whole. “Radiologist must get involved”, she insists. “They must assume the role of a specialist in image guided therapy – a therapeutic discipline of its own Radiologists must sit in multi-disciplinary conferences in order to be accepted as a clinical partner who has a saying in the therapeutic management of patients.”. The success speaks for itself: Already during her first six months as Chairman of Radiology at the UKA, the number diagnostic procedures, but in particular that of therapeutic interventions, have increased substantially.
The radiologist is particularly conscious that minimally invasive treatment can only be facilitated through interdisciplinary cooperation. ‘With my young colleagues there is no garden fence mentality, where people work in their own silos. Our working life is characterised by many meetings and lively tumour board discussions. Thanks to brief communication, and coordination times, we can offer patients a comprehensive same-day service from diagnosis to starting treatment.’ The expert in oncologic imaging obviously also brings her personal note to the role through extensive experience in MR imaging: ‘MRI is like a grand piano – you have to learn to play it first before it makes the desired sound.
Obviously, nothing will happen without the right technology, either. Prof. Kuhl’s first step was to have her entire equipment for breast cancer diagnosis moved from Bonn to Aachen. A 1.5-Tesla Philips Achieva MRI scanner was available at Aachen. Her breast patients have followed her to the UKA because they come from all over Germany, anyway, and because they want to meet the undisputed expert in the field of breast cancer diagnostics. .
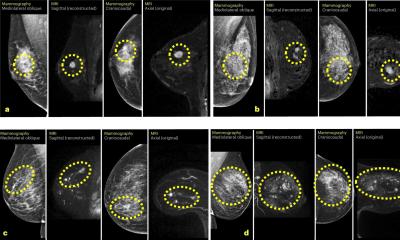
Christiane Kuhl is an internationally respected advocate of breast MRI . She has proved the superior sensitivity and specificity of MRI compared to mammography and ultrasound in numerous pieces of research, most recently in the EVA Study (Journal of Clinical Oncology; doi: 10.1200/JCO.2009.23.0839), for which over 700 high-risk patients were examined by MRI, mammography and ultrasound between 2002 and 2007. The study showed that MRI not only had by far the highest detection rate for breast cancer (93%) but also made an additional mammography or ultrasound examination redundant.
With these findings, Prof. Kuhl has not only made friends, but also attracted considerable criticism for her contrarian approach, particularly from advocates of mammography screening programmes. ‘We’ve known for many years that MRI is required to allow an early diagnosis of breast cancer, particularly in the case of young women who are at increased risk of developing breast cancer,’ she pointed out. “So MRI should be considered the cornerstone of screening young women at elevated familial risk of breast cancer. And since the EVA trial, we know that, if MRI is available – then a mammogram is indeed redundant. So the guidelines should be changed accordingly to reflect this. Yet the findings are being ignored or treated almost as blasphemy”. This is in spite of the fact that there are no scientific data on the use of screening mammography for women under the age of 40 anyway” she underscores. “
In this age group, mammography ought to be treated as an experimental procedure in the same way as MRI or ultrasound.’ And she added: ‘Particularly in the case of women with a mutation of the tumour suppressor gene BRCA1, the ionising radiation associated with a mammogram may even favour tumour development.
Prof. Kuhl’s fight for breast MRI has now borne fruit in the USA: The American Cancer Society has changed its guidelines on the early detection of breast cancer and generally recommends MRI as the method of choice for the early detection of breast cancer in women at elevated risk of developing the disease. “The ACS recommends breast MRI screening for every woman with a lifetime risk of 20% and higher. This is not a “high risk” situation – it is just slightly higher than the average risk, i.e. 15% lifetime for women in western European countries”, she says,
As MRI can visualise very small lesions, Prof. Kuhl depends on having MR guided vacuum-assisted biopsy at her fingertips. For MRI guided biopsy she is supported by the ATEC Biopsy System from Hologic: ‘A particular progress with this generation of equipment is that it generates a strong vacuum. This means that even the smallest lesions in the most unfavourable places (e.g. pre-pectoral location) can be sampled without any difficulties. Because of the continuous flushing of the biopsy system, it is easy to precisely delineate the biopsy cavity. This improves the control of the biopsy procedure as a whole and reduces by half the actual time spent on the examination table.’
Prof. Kuhl sees a further technical advantage in the development of variable coil geometry for MRI breast imaging. ‘Every breast is different – and they come in different sizes – something that the engineers of new coil technology should surely be able to understand,’ she said, somewhat tongue-in-cheek. Instead of one-size-fits-all breast coils the trend is towards smart coils, which are built directly into the compression plates and are thus suitable for different breast sizes. This has a significant advantage for smaller breasts. ‘Small breasts have little fatty tissue and consist virtually of densely packed glandular tissue. Therefore, small breasts tend to exhibit fast and strong enhancement ,’ she explained. ‘This is why small breasts are usually MRI-“dense” breasts, which means that we need to image very quickly in order to detect breast cancer. However, this is difficult: “Small, non-fat breasts do not contain many protons. Fast imaging is difficult because this may yield borderline signal to noise. To account for this and again increase signal-to-noise, it would be helpful if the coils can be positioned very close to the breast, i.e. within the compression plates.
Compression, however, must be done in the slice encoding direction, i.e. in the feet-head-direction for axial imaging, and in the medio-lateral direction for sagittal imaging. Compressing the breast in the slice encoding direction serves several purposes: It reduces motion, but it also reduces the number of sections needed to cover the entire breast. Especially for 2D gradient echo MR imaging protocols, a reduced number of sections translates into faster acquisition times – and it also means that we have to review only between 25 and 29 sections’
So far, variable coil geometry has only been offered for the American market by Sentinelle Vanguard. Because US radiologists prefer sagittal imaging, the compression is so far only in the medio-lateral direction. “This is not useful for the European market, i.e. for axial imaging. With axial imaging, compressing the breast in the medio-lateral direction even increases the number of sections needed to cover the breast, and it is a poor use of the field of view because the breast appears squeezed like a lemon and occupies only a small fraction of the entire image”..
Asked when she is thinking of taking up her scientific research with explicit ‘explosive force’ at the UKA, the radiologist raised her hands disarmingly. ‘Currently there’s no time for this. Most people only know me for my research and forget that I also have a daily, routine clinical and administrative working life to contend with – as director of a Department now more than ever. Therefore, I’m quite pleased that my reputation does not precede me in Aachen. Many of my colleagues here don’t even know what I’ve done in the past. For now I’m just happy enjoying this.’
14.03.2011