Image source: Vogl TJ, Bielfeldt J, Kübler U, Adwan H; Cancers 2024 (CC BY 4.0)
Article • Freezing cancer cells
Cryoablation: A treatment option for low-risk early-stage breast cancer
Cryoablation, the destruction of malignant cancer cells by freezing them, is increasingly becoming an alternative to having conventional lumpectomy for patients diagnosed with early-stage, localised, low-risk breast cancer. Findings from numerous recent clinical trials show that cancer recurrence rates are very low and are comparable to breast conservation surgery (BCS).
Report: Cynthia E. Keen

Photo courtesy of IceCure
Mild-to-moderate adverse effects for patients having the procedure include bruising, localised edema, freeze-related skin burns, rash, bleeding from needle insertion, local hematoma, tenderness, pruritis and rash. They resolve rapidly without complications or long-term residual effects.
‘Cryoablation is most effective when treating small lesions without extensive intraductal component,’ say Lauren M. Kopicky, MD, a breast surgeon at Cleveland Clinic and Debra A. Pratt, MD, Medical Director of breast services of the Moll Cancer Center of Fairview Hospital in Ohio.1 They caution that breast cryoablation is appropriate only for select patients, and is currently authorized by the US Food and Drug Administration (FDA) only in clinical trials. According to cryoablation technology developer IceCure Medical, the technique is approved for use in Europe for breast cancer and fibroadenomas (benign breast tumours) for over two decades and is considered a well-tolerated outpatient procedure.
Unlike in BCS, however, no breast tissue is removed, and scarring is minimal. The procedure is performed in outpatient hospital radiology departments, with local anaesthesia and ultrasound or MRI guidance, taking less than an hour. Patients experience little discomfort and can resume normal activities within a day or two.
Promising trial results
Much awaited five-year outcomes of the ICE3 Trial, initially presented at the 2024 American Society of Breast Surgeons (ASBrS) Annual Meeting, may spur FDA approval.2 This is the first and largest-to-date prospective, multi-centre clinical trial of breast cryoablation for breast cancer. One hundred ninety-four women, ages 55 to 94, received cryoablation treatment at 19 hospitals, with imaging follow-up only and no subsequent tumour excision for 194 patients. None had lymph node involvement. Almost 80% of participants received adjuvant treatment, predominantly (63.9%) endocrine treatment.3 Seven patients (3.7%) experienced cancer recurrence. Two patients (1%) developed distant metastasis and died.
Principal investigator Richard E. Fine, MD, of the West Cancer Center and Research Institute in Germantown, Tennessee, reported that at 54 months, the overall ipsilateral breast tumour recurrence (IBTR) rate was 3.7%, 3.2% for patients who subsequently received endocrine surgery. This gives a five-year IBTR survival rate of 4.3% and 3.7%, respectively. Five years following treatment, 100% of patients and physicians were very satisfied with cosmetic results: a normal-looking breast with a small scar from the cryoablation needle.
CT-guided cryoablation for curative intent and metastatic local tumour control
In Germany, cryoablation is being used to treat patients with localised recurrence, auxiliary node involvement, and metastasis. Researchers at University Hospital Frankfurt report their treatment of 56 tumours in 45 patients using liquid-nitrogen based CT-guided cryoablation in Cancers.4
The study cohort consisted of breast cancer patients who did not want to undergo surgery or who had unresectable tumours who underwent cryoablation between May 2019 to May 2023. They ranged in age from 31 to 86 years. Thirteen with newly diagnosed breast cancer and 11 with breast cancer recurrence were treated with curative intent. Twenty-one with metastases were treated for local tumour control. All patients completed the treatment, and none experienced any complications.
Recommended article
Article • Alternative to lumpectomy
Breast cryoablation for surgically inoperative patients
Breast cryoablation is an emerging treatment for early-stage, localized breast cancer that destroys malignant tumours by freezing them. During the past decade, it has been increasingly utilized as an alternative to lumpectomy, but its long-term benefits compared to other breast cancer treatments are still unproven.
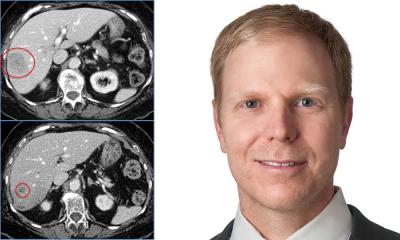
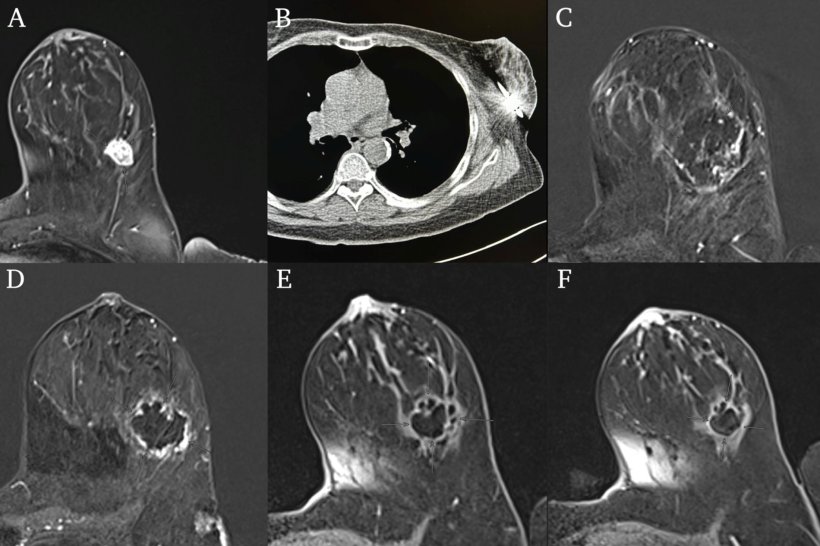
Patients had a planning CT-scan prior to cryoablation to locate an appropriate incision point and plan the trajectory of the cyroprobe shaft. Breast MRI scans were performed 24-hours post-treatment. If any residual contrast-enhanced tumour tissue was seen at ablation margins, another cryoablation procedure was performed to ensure complete ablation of the tumour.
Principal investigator Prof. Thomas J. Vogl, MD, PhD, Director of the Clinic of Radiology and Nuclear Medicine, and colleagues advise that they selected CT-guidance instead of ultrasound guidance for the ablation procedure to enable an exact visualisation of the cryroprobe, the malignant tumour, and the ice ball in all dimensions and to ensure a sufficient safety distance to adjacent structures. They say that the advantages of using a liquid-nitrogen system are that it is cost-effective, time-efficient for both patient and clinicians, and has a notably better cosmetic outcome. It does not require specific security measures, because liquid nitrogen is not stored in a pressurised container. The disadvantage is that the procedure takes considerably longer than either microwave or radiofrequency ablation procedures.
Profiles:
Richard E. Fine, MD, is a breast surgeon at the Margaret West Comprehensive Breast Center in Germantown, Tennessee. He has the distinction of being one of the first surgeons in the United States to perform image-guided breast biopsies and has extensive experience in new breast biopsy methods. Dr Fine is a past president and Chairman of the Board of the American Society of Breast Surgeons.
Prof. Thomas J. Vogl, MD, PhD, an interventional radiologist, is Director of the Clinic of Radiology and Nuclear Medicine at University Hospital Frankfurt, Germany, specializes in interventional oncology and vascular procedures. He also is Professor for X-ray Diagnostics of the Goethe University Frankfurt am Main. Dr Vogl’s research has resulted in worldwide optimisation of imaging procedures and surgical methods. He was involved extensively in the evaluation of contrast agents and developed an angiography robot with the ability to deliver high-resolution diagnostic images from inside the body to detect previously undiscovered tumours.
References:
- Kopicky LM, Pratt DA. Cryoablation and Breast Disease. Curr. Breast Cancer Rep. 2024. 16:279-287.
- Fine R, Gilmore R, Dietz J, et al. Cryoablation without Excision for Early-stage Breast Cancer: ICE3 Trial 5-year Follow-up on Ipsilateral Breast Tumor Recurrence. Scientific session 176458, 25th ASBrS Annual Meeting. April 2024.
- Fine RE, Gilmore RC, Tomkovich KR, et al. Cryoablation Without Excision for Early-Stage Breast Cancer: ICE3 Trial 5-Year Follow-Up on Ipsilateral Breast Tumor Recurrence. Ann Surg Oncol. Published online 16 September 2024.
- Vogl TJ, Bielfeldt J, Kübler U, et al. CT-Guided Percutaneous Cryoablation of Breast Cancer: A Single-Center Experience. Cancers. 2024 16, 2373.
20.03.2025