Photo: supplied
Article • Ovarian cancer and endometriosis detection
Women’s health imaging: PET/CT and T2*w MR show promise
Diagnostic imaging in women’s health advances: Positron emission tomography–computed tomography (PET/CT) might provide a more accurate imaging alternative to CT in ovarian cancer. T2*-weighted MR imaging in deep endometriosis detection also shows promise, but ultimately falls flat. In a dedicated session at the ECR 2022 Overture in March, experts presented their latest research projects.
Report: Mélisande Rouger
Photo: supplied
Dr Elaine Yuen Phin Lee from the Department of Diagnostic Radiology at the University of Hong Kong talked about monitoring treatment response in epithelial ovarian carcinoma (EOC) with PET/CT following neo-adjuvant chemotherapy (NACT). ‘EOC presents late as advanced-stage disease because early-stage disease tends not to present symptoms,’ she said. ‘Cytoreduction remains the most effective treatment and the ability to achieve complete cytoreduction is prognostic for survival.’
To achieve cytoreduction, the patient can either undergo upfront cytoreduction or NACT, followed by interval debulking surgery. Treatment response to NACT is currently assessed by CT, but this may not be accurate all the time, Lee explained. ‘The diagnostic accuracy of CT has quite a wide range, in between 57 to 94% depending on the study you look at. Mostly, this is limited by subcentimetre lesions and immeasurable disease, which is common in advanced stage carcinoma,’ she said.
Metabolic change detection for early diagnosis
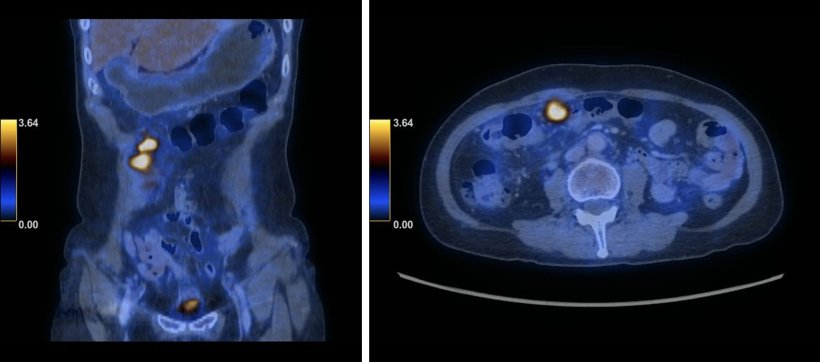
By comparison, PET/CT offers accuracy rates that are consistently high, with reported figures of 90-95% in primary evaluation of EOC. The reason for this is that PET/CT picks up on the metabolic changes in the patients, which occurs earlier than the anatomical changes that are detected via CT, Dr Lee said. ‘Unfortunately, there’s a lack of data on the diagnostic accuracy of PET/CT in the setting of NACT in EOC.’ The expert and her team thus hypothesised that metabolic activity in these tumour deposits on PET/CT could increase the visual conspicuity of the tumours and diagnostic accuracy after NACT in EOC.
The objective of the study Dr Lee presented at ECR was to evaluate the accuracy of PET/CT in monitoring treatment response in EOC after NACT. ‘We recruited 15 patients with stage III to IV of EOC who were scheduled for NACT and PET/CT after 3 cycles of NACT before interval debulking surgery,’ she explained. For PET/CT evaluation, the researchers divided the abdominopelvic cavity into 19 regions and used a 5-point Likert scale to score the evaluation, with 1 signifying the absence of disease and 5 being malignant. Region-based analysis was performed subsequently.
Recommended article

Article • Underrated technique
Pitfalls in pelvic CT imaging
Computed tomography (CT) plays an increasingly important role in assessing pelvic disease, particularly when patients present with acute abdominal pain. In addition, radiomic approaches on CT are being developed to increase the characterisation of ovarian cancer for optimising treatment planning.
Metabolic change detection for early diagnosis
Lee and her team also used histopathological correlation as gold standard, and in the instances in which biopsy resection could not be performed, they took the surgical evaluation as standard. They evaluated 285 regions with an accuracy of 88%, but low sensitivity at 38% and high specificity at 96%. Positive predictive value (PPV) was low at 56% while negative predictive value (NPV) was high at 91%.
This preliminary study showed that PET/CT achieves low sensitivity in all regions, but high specificity and NPV. Exceptions were found in two regions in the omentum, because of the presence of microscopic disease that could not be picked up on PET/CT, and also in the central pelvis because of low spatial resolution on both CT and PET examinations. ‘PET/CT is highly specific with high NPV in treatment response assessment after NACT in EOC,’ Lee concluded. Taking into account the relatively small sample size, she proposed that PET/CT might be useful in surgery planning, allowing for disease stratification to assess the viability of less aggressive and debulking surgery.
Endometriosis: A closer look at blood degradation products

Photo: supplied
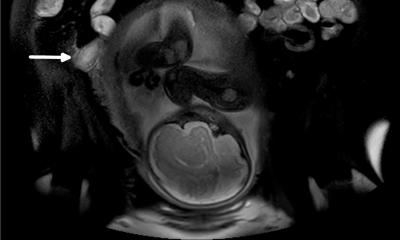
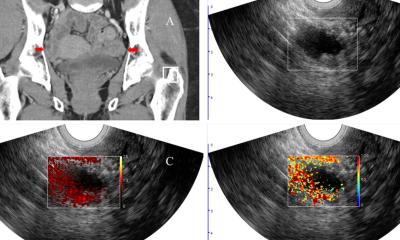
In the following talk, Dr Paolo Niccolò Franco from the Department of Diagnostic Radiology at Papa Giovanni XXIII Hospital in Bergamo, Italy, shared the results of a study comparing T2*-weighted vs. standard MR imaging performance in detection of deep endometriosis. ‘Endometriosis is a chronic gynaecological disorder characterised by the presence of ectopic functional endometrial tissue outside the uterine cavity,’ he said. ‘This condition affects approximately 10% of women of reproductive age. Deep infiltrative endometriosis is defined as the presence of implants extending 5 mm or deeper under the peritoneal surface.’
MRI has been shown to be an effective tool for both diagnosis and treatment planning of deep pelvic endometriosis. T2*-weighted sequences are susceptible to chronic blood degradation products – such as hemosiderin – which are visualised as signal voids. To take advantage of this, it has recently been proposed that these sequences can provide added value to detect ectopic endometrium by identifying hemosiderin deposited during cyclic bleeding.
The aim of Dr Franco’s study was to evaluate the diagnostic performance of T2*-weighted sequences, compared to conventional pelvic MRI protocol, in the detection of deep pelvic endometriosis. The researchers enrolled 44 patients who underwent a pelvic MRI on a 3T scanner for clinical and/or ultrasound suspicion of deep endometriosis.
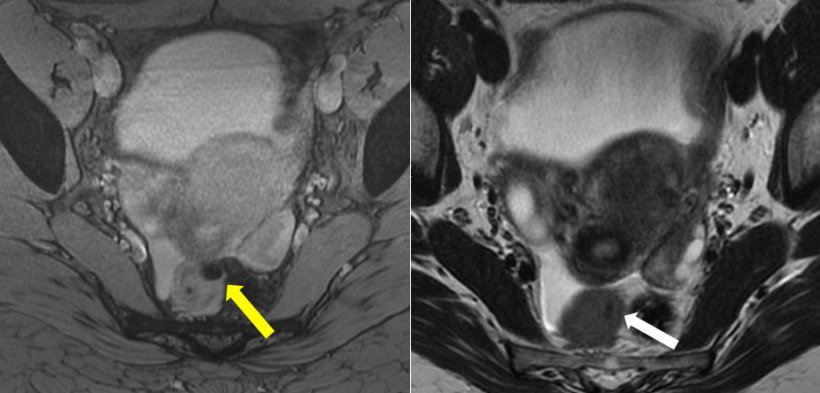
Photo: supplied
T2*w MRI prone to diagnostic overestimation
Three readers independently evaluated MR images. The first reader was a staff radiologist with ten years’ experience, who analysed images taken with both conventional MRI protocol and T2*w sequences. The second reader, a resident with 2 years’ experience, analysed conventional sequences. The third reader had limited experience and analysed images taken with both conventional MRI protocol and T2*w sequences. The first reader diagnosed endometriosis lesions mainly in the ovaries, the torus uterinus, retrocervical space and the utero sacral ligament. The first two readers agreed on endometriosis sites on both conventional protocols and T2*w sequences. ‘The number of lesions detected by the third reader on T2*w sequences was significantly higher, mainly because the reader mistook some findings for endometriosis lesions, for example gas in the vaginal fornix and rectal lumen or artifacts caused by caesarean scars,’ the expert said.
T2*w sequences do not seem to bring added value to expert readers in their assessment of endometriotic lesions, Dr Franco concluded. ‘Artifacts caused by undesirable sources of magnetic signal voids may lead to diagnostic overestimation, especially for readers with limited experience.’
Profiles:
Following her radiology training in the UK, Elaine Lee joined the Department of Diagnostic Radiology, Li Ka Shing Faculty of Medicine, University of Hong Kong in 2010 and is now a Clinical Associate Professor. She has subspecialty interest in gynae-oncology, specifically in the application of functional and molecular imaging techniques. She is the primary investigator and recipient of competitive national grants in advancing the research in gynae-oncology imaging. She enjoys post-graduate mentoring and undergraduate teaching.
Dr Paolo Niccolò Franco was born in Cosenza, Italy, and obtained his medical degree at the University of Florence. He is a fourth-year resident at the Post-Graduate School of Diagnostic Radiology of the University of Milano-Bicocca and his residency was at San Gerardo Hospital in Monza and Papa Giovanni XXIII Hospital in Bergamo. He has a special interest in pelvic, genitourinary, and gynaecological imaging. Dr Franco is a member of the European Society of Radiology and the Italian Society of Medical and Interventional Radiology.
21.04.2022