

Interview • Cardiac imaging on ICE
The benefits of Intracardiac echocardiography
Intracardiac echocardiography (ICE) is an increasingly important guiding tool for structural heart disease interventions – without general anaesthesia. José Ribeiro, who works in the thorax and circulation unit at Gaia Hospital Centre, Portugal, who has worked with this technology for the past two years, explained its benefits and limitations.
Interview: Daniela Zimmermann

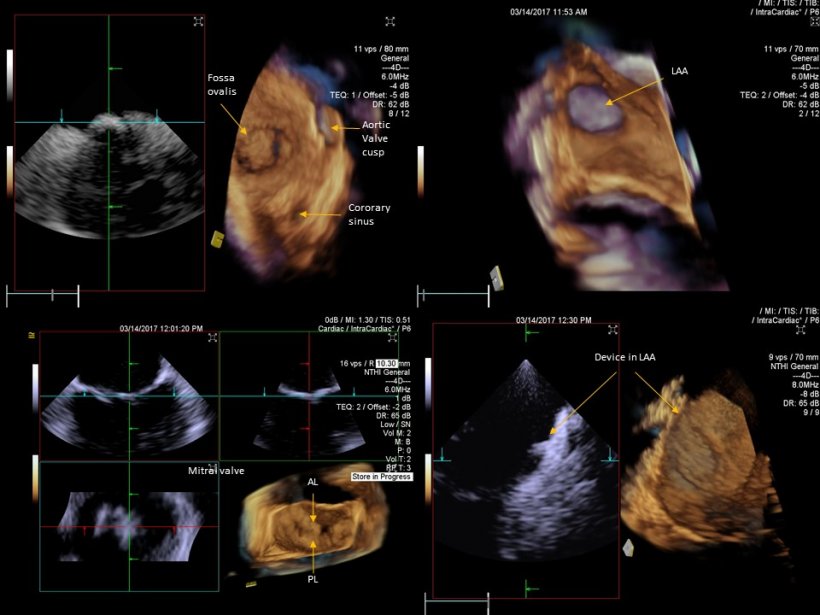
Discussing developments in Intracardiac echocardiography (ICE), José Ribeiro, cardiologist at the thorax and circulation unit in Gaia Hospital Centre, Portugal, explained that recently the need for a different ultrasound tool to guide patient treatment beyond transoesophageal echocardiography (TEE) became clear. ‘Consequently,’ he added, ‘a significant number of interventional cardiologists have started to use ICE. ‘We still have limitations with ICE for structural heart disease, because we don’t see all the structure in the same plan and need to navigate with a catheter inside the heart. That’s why it’s so important for 3-D imaging to guide procedures. ‘We don’t need too much imaging to guide the intervention for structural heart disease. But we need to have a good pre-procedure evaluation and to plan the procedure, and after that we only need specific steps to ensure procedure quality and check the results. If we can get the cardiac structures on 3-D, we have a significant advantage for guidance. We initially had a narrow angle catheter, which only enabled us to view small volumes of the heart. This is not enough to image entire structures, for instance a valve, left appendage or oval fossa. So we developed a new device with a wide opening angle; it’s a 12.5-Fr catheter and this enables us to view significant volumes of the cardiac tissue, including the whole mitral valve. This development appears to be a great advantage for guidance.’
HiE: When using ICE, is the image in front of you and can you see the relation between the structures?
José Ribeiro: Yes. When we have a volume, we can look inside and decompound it in a different 2-D plan to navigate more easily, which enables us to be more confident when doing the procedure. With a 3-D wide angle ICE catheter, we have the same benefits as with 2-D ICE, meaning we don’t need an anaesthetist, the interventional cardiologist can do the intervention him- or herself, by putting the catheter in the right place to see the heart. But we can also obtain a significantly higher amount of information and anatomy, so that the interventional cardiologist can do the whole procedure without having to navigate with the image catheter. We can put the catheter in the right place, and then we don’t need to move it to see what we need to see.
What are the benefits of not having to move the catheter?
Moving the catheter to view the cardiac structures means more work, more time, more risk and more radiation. In the interventional lab, we always use angiography and ultrasound. Angiography, i.e. radiation imaging, helps us to carry out the procedure and navigate to place the ICE catheter inside the heart. If we don’t need to move the catheter because we can see everything at once we of course also need less radiation. If we have a technology that gives us everything with the catheter in the same place, it’s much better.
Many specialists are needed in such an intervention. One day, could just one person do this?
With ICE, we can do everything while the patient is awake, without discomfort and anaesthesia, and with fewer people inside the room and less radiation
José Ribeiro
That’s the big point. But we need to train interventional cardiologists, to change their mind-set. They typically use angiography and ignore ultrasound. However, this is changing now. Everything is changing in the interventional lab. We are using TEE in a significant number of procedures; but with TEE we also need specialists. With ICE, we can do everything while the patient is awake, without discomfort and anaesthesia, and with fewer people inside the room and less radiation.
In the lab, for ICE guidance we use the echocardiography machine to direct the image and ICE catheter manipulation beyond the angio room equipment. In future, we could have all the controls on the table – connecting angio and ultrasound controls. Also, we need to improve the imaging display software, with specific play sets for detailed procedures, to give the right plans for each interventional procedure. Right now, in our hospital, we simultaneously use display ultrasound imaging and angio imaging on the same screen. We can switch to all the positions we need, but we need lots of training to be able to see it. The learning curve for interventional cardiologists is long. Some interventional cardiologists already have experience with 2-D imaging, and they have a significant advantage to give the final step to use 3-D imaging in ultrasound. The learning curve is more important when you are using angio only.
For which cases do you use TEE and ICE?
In our lab we check all patients in the echo lab in a selection process and, when we are very confident about the pathology or anatomy, we use the ultrasound image (TEE or ICE) for guidance and to improve confidence during the procedure. In simple cases, such as ASD or PFO closure, we use ICE. As mentioned earlier, ICE gives us many advantages - no anaesthesia needed, more comfort, etc. For more complex cases we must decide how much imaging we need. We also use ICE in normal mitral valve repair; we have initial experience with this wide angle 3-D ICE catheter that crosses the inter-atrial septum to scan left side structures, for instance.
So far, our experience with ICE is limited. But even with more experience, in complex cases we tend to prefer the technique or imaging tool with which we have more experience. So TEE may still be preferred in such scenarios. The main limitation of ICE is lack of experience with the technology. In addition, if the case is too complex, we may need to cross with the catheter to the left side, so we need to move the catheter to be sure. ICE could be useful in some patients who cannot be imaged with TEE. Both methods are alternative. ICE is a step forward, especially with this new dimension – 3-D ICE. But,’ he concluded, ‘in the future we need to check what’s the best option for each patient.
Profile:
José Manuel Coelho Ribeiro MD directs the Thorax and Circulation Unit at Vila Nova de Gaia Hospital Centre in Portugal. Having graduated from Oporto medical school in 1992 he became a cardiology specialist in 1996, which was followed by an echocardiography fellowship at Onze-Lieve-Vrouwziekenhuis in Aalst, Belgium. He also became a member of the Portuguese Cardiology College. Since 2001, he has led the echo lab (with 9,600 studies in 2017) and, from 2006, has been cardiology consultant in the Espinho Hospital Centre at Vila Nova de Gaia, where he has implemented new techniques, including transoesophageal echocardiography, as well as coordinated several telemedicine projects.
27.08.2018


