Image courtesy of Prof. Galea
Article • A call for consistency at ECR 2026
The aorta is an organ now – and radiology needs to catch up
As the aorta gains recognition as a functioning organ rather than a simple blood conduit, the lack of standardised imaging protocols is becoming an increasingly pressing concern. At ECR 2026 in Vienna, Professor Nicola Galea from Sapienza University of Rome made a compelling case for unified imaging approaches, warning that inconsistency in measurement techniques can lead to flawed clinical decisions.
By Mark Nicholls

Image courtesy of Prof. Galea
Galea, an Associate Professor in Radiology at the Department of Radiological, Oncological and Pathological Sciences, described the aorta as 'an organism with specific vital function'1 – far more than a passive tube transmitting blood from the heart to the rest of the body. 'There is an increasing emphasis on considering the aorta not as a simple conduit that transmits the blood from the heart to the rest of the body, but like a functional organ,' he told delegates.
Yet while the number of papers and guidelines on the aorta continues to grow, most devote little attention to imaging requirements. Session chair Professor Hatem Alkadhi from University Hospital Zurich set the scene by noting that 'there are so many guidelines about the aorta from so many societies' but only a few from radiological groups. 'What they all do have in common,' he continued, 'is that they consider the aorta to be an organ, and should be approached like this, which has consequences for both imaging and reporting.'
Speaking in the session entitled Approaching the Aorta as an Organ, Galea specifically focused on standardising aortic imaging and assessment, covering appropriate approaches for aortic imaging, standardised post-processing and measurement methods, and ways to minimise inter-reader and inter-study variability.
When millimetres shape clinical decisions
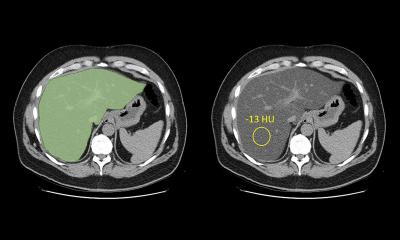
As modern healthcare management becomes increasingly image-driven, guidelines rely more and more on diameter thresholds and indexing measurements. 'That means clinical decisions may depend on small differences, but small differences can have a huge impact in the management of the patient,' Galea explained. 'But the guideline documents do not say how and where to measure, and there is no detail on techniques to apply, how to study a patient, and report.'
Aortic imaging, he noted, is 'inherently variable' from a technical point of view, in methodology, and in reader experience – and can be further influenced by the approaches of a specific institution. Artificial intelligence may also play a role. 'As a result, lack of standardisation leads to clinical inconsistency,' he said.
The consequences can be significant: 'Comparable studies can give artificial changes in aortic measurement with false interpretation in the progression and stability of disease and when an assessment is not reproducible that can result in a different therapeutic strategy on the same patient.' This may also lead to physicians losing confidence in radiological reports and conducting their own measurements and assessments.
ESCR consensus document in the works
To address this lack of consistency, Galea reported that the European Society of Cardiovascular Radiology (ESCR) is working on a consensus document offering recommendations on diagnostic definition criteria and standard reporting. Elements covered include guidance on modality selection, scanning protocols, quantitative aortic assessment, and reporting standards.
Standardised definitions are essential to reduce diagnostic ambiguity and standardisation reduces variability in clinical decision making
Nicola Galea
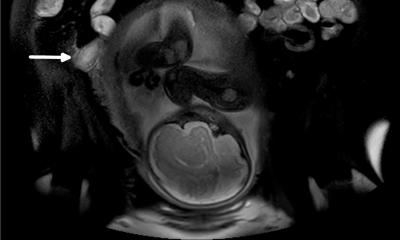
Recognising the 'rich toolbox' of imaging modalities available, Galea identified computed tomography angiography (CTA) as the standard for measuring and assessing aortic disease, especially in emergency settings. 'Ultrasound is a first line modality and MRI can be reserved for paediatric patients, young adults, or during pregnancy, and nuclear medicine has a role especially in patients with inflammatory disease, or infective disease.'
In the context of aortic imaging with CTA, he stressed that ECG gating is mandatory when evaluating the aortic root.
Consistent terminology as a foundation
Galea emphasised the importance of an accurate definition of aortic pathology for appropriate clinical management. 'Standardised definitions are essential to reduce diagnostic ambiguity and standardisation reduces variability in clinical decision making,' he concluded.
His final message was clear: dedicated protocols with full aortic coverage are critical; accurate and reproducible techniques should be used to standardise measurements; and consistent terminology must be adopted for aortic pathology.
Profile:
Professor Nicola Galea is a cardiovascular radiologist and Associate Professor in Radiology at Sapienza University of Rome, Italy. He heads the Cardiovascular CT & MR Imaging Unit at the Policlinico Umberto I Hospital. His research focuses on advanced cardiac imaging – particularly cardiac magnetic resonance, 4D Flow aortic imaging, the impact of surgery on aortic morphology and dynamics, as well as imaging biomarkers in cardiomyopathies and inflammatory or ischaemic heart disease.
Reference:
14.07.2026