Article • Choosing the right modality for expectant mothers
Abdominal imaging in pregnancy: Balancing diagnostic accuracy with fetal safety
Imaging pregnant women with acute abdominal pain remains a significant clinical challenge – not only because of concerns about the impact on the unborn child, but also due to the anatomical changes that can obscure diagnosis. At the European Congress of Radiology (ECR) in Vienna, radiologists Vikas Shah and Charis Bourgioti examined the protocols for safe imaging in pregnancy and the management of abdominal emergencies in expectant mothers.
By Mark Nicholls
Image source: Bufman H, Raskin D, Barash Y et al., PLOS One 2024 (CC BY 4.0)

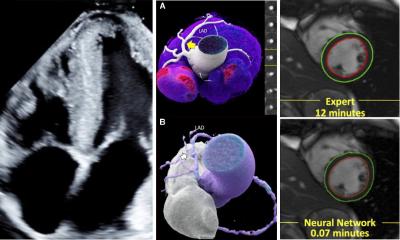
Image source: ESR
Diagnosing acute abdominal pain in pregnant women is fraught with difficulty, explained Vikas Shah, a consultant radiologist at University Hospitals of Leicester NHS Trust. Normal physiological changes in pregnancy – such as tachycardia and the displacement of anatomical structures by the enlarging uterus – can mimic the signs of acute inflammatory disorders, making clinical assessment unreliable.
'Many of the normal findings of pregnancy overlap with those features that you find in acute inflammatory disorders such as tachycardia, making a clinical diagnosis difficult,' he said. 'As the uterus enlarges, there is also displacement and compression of normal anatomic structures.' Even when imaging is clearly needed, uncertainty can cause hold-ups, Shah warned: 'There can also be some delays because of hesitancy in knowing how to perform a study or perhaps lack of local protocols or pathways. Such delays ultimately lead to harm.'
Weighing up the imaging options
In his ECR presentation, Shah explained that diagnosing acute abdominal pain in pregnant women is fraught with difficulty.
While ultrasound is widely available and low-cost, Shah noted that anatomical changes in pregnancy make it 'very difficult particularly in the second and third trimesters.' CT, though commonly used for abdominal emergencies, raises concerns about radiation and contrast exposure. MRI, however, offers what Shah described as 'the best of both worlds' – radiation-free, multi-planar cross-sectional imaging with high sensitivity and specificity. 'It has a high sensitivity and specificity and high inter-observer concordance, which means radiologists of varying level of experience can reliably report MRI studies,' he said.
Shah discussed the use of 1.5T scanners without intravenous or oral contrast, highlighting the benefits of diffusion-weighted imaging (DWI) for detecting inflammatory change and Fast Spin Echo (FSE) T2 sequences for identifying anatomy, masses, and oedema.
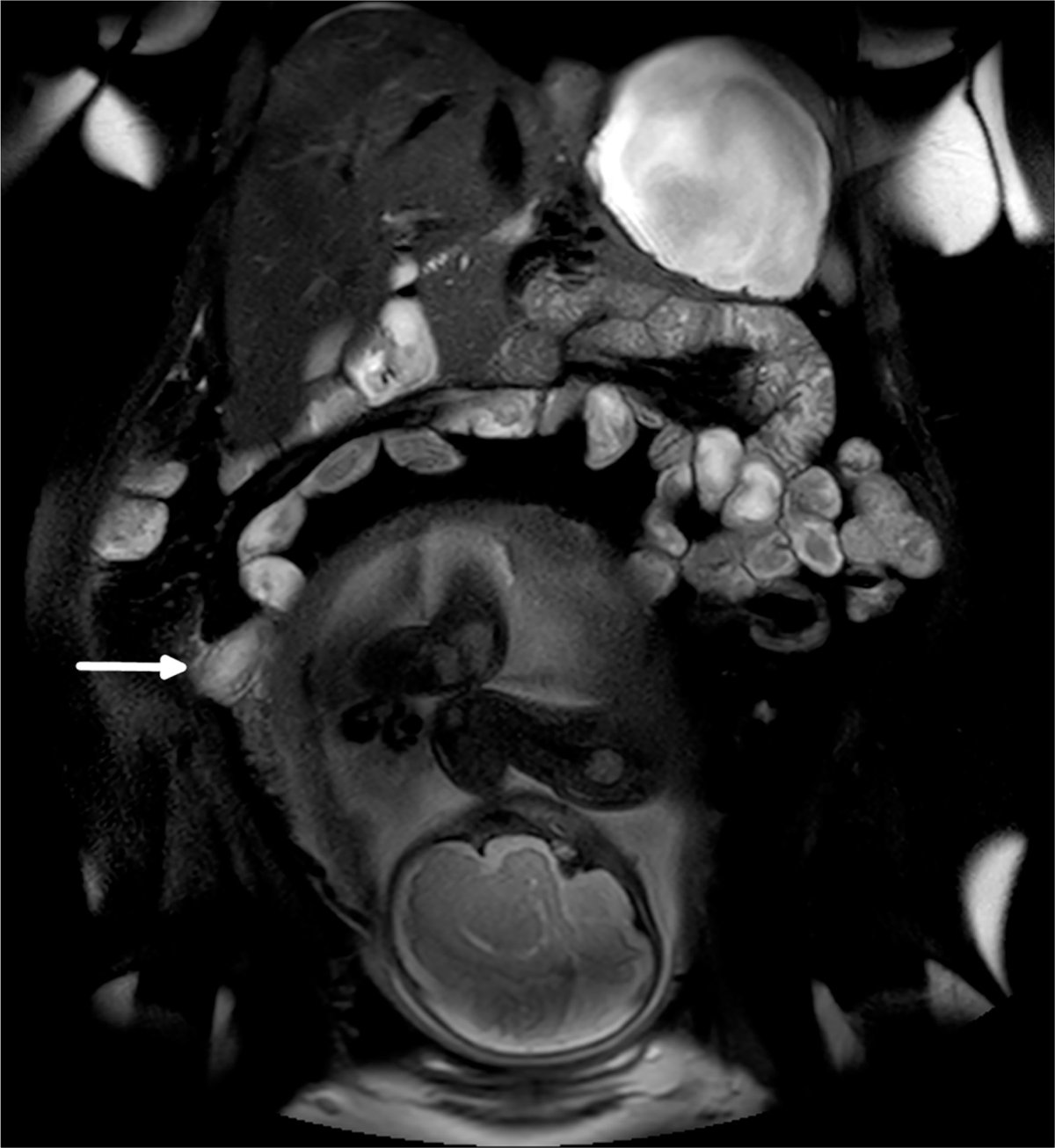
Image source: Bufman H, Raskin D, Barash Y et al., PLOS One 2024 (CC BY 4.0)
Appendicitis is the most common non-obstetric surgical emergency in pregnancy, affecting 1 in 1,500 pregnancies. Shah warned that uncomplicated appendicitis in early pregnancy can lead to fetal loss rates of up to 2% – a figure that rises with diagnostic delay.1 'That shows the importance of imaging in both accuracy and timeliness. We need to get the diagnosis right because a negative appendectomy will increase fetal loss rate,' he said.2 'We also need to scan on time because a delay in making a diagnosis will lead to perforation, abscess formation, and an increase in the fetal loss rate.'3
Beyond appendicitis, Shah outlined the role of imaging in identifying renal masses, non-haemorrhagic adrenal infarction, ovarian hyperstimulation, ectopic and heterotopic pregnancies, and fibroid degeneration. He stressed that DWI has particular value in leading clinicians to potential abnormalities. 'It is important to use a standard imaging protocols for all cases. The aim is to think beyond the appendix and review other organs carefully. A prompt diagnosis is very important in preventing fetal loss,' he said.
Optimising protocols for safe imaging

Image source: ESR
Charis Bourgioti, Assistant Professor of Radiology at the National and Kapodistrian University of Athens, addressed the optimisation of imaging protocols in pregnancy, covering CT and MRI safety issues for mother and fetus, and indications and contraindications for contrast agents.
She emphasised the need to consider medical, psychological, and legal-ethical dimensions: 'The diagnostic work-up should be restricted as a general rule to those methods that do not endanger fetal health, and only absolutely necessary radiological interventions are justified, especially during the first trimester.'
While ultrasound and MRI remain the preferred modalities due to the absence of ionising radiation, Bourgioti maintained that all imaging modalities can be used 'if it is clinically indicated'. However, she cautioned that persistent confusion over safety 'results in unnecessary avoidance of useful diagnostic tests.'
Balancing benefit and risk
Sonography has no known adverse effects on the developing fetus and serves as a primary screening tool, while MRI provides excellent soft-tissue contrast. Pregnant patients can be safely imaged at field strengths of up to 3T, though 1.5T is preferred – especially in the first trimester.4
Bourgioti advised that ionising radiation is best avoided in pregnancy, with CT reserved for situations where ultrasound or MRI cannot provide the required information.5 The use of contrast agents should be limited, she said, as 'their effects on the human embryo or fetus are incompletely understood',6 and gadolinium should only be administered 'if the potential benefit exceeds the potential risk.' She also noted that, according to new recommendations, abdominal shielding offers limited benefit, as most of the fetal dose comes from internal scatter.7
Profiles:
Dr Vikas Shah is a UK-based consultant radiologist at University Hospitals of Leicester NHS Trust, and managing editor of Radiopaedia. He specialises in abdominal, emergency and post-mortem imaging. He is an Honorary Associate Professor at the University of Leicester and the Undergraduate Radiology Lead for the Leicester Medical School.
Dr Charis Bourgioti is Assistant Professor of Radiology at the National and Kapodistrian University of Athens, Aretaieion Hospital, Greece. She specializes in women's imaging and obstetrical MRI, with a particular focus on placental and maternal pathology.
References:
- Theilen LH, Mellnick VM, Shanks AL et al.: Acute Appendicitis in Pregnancy: Predictive Clinical Factors and Pregnancy Outcomes; American Journal of Perinatology 2017; https://doi.org/10.1055/s-0036-1593764
- McGory ML, Zingmond DS, Tillou A et al.: Negative appendectomy in pregnant women is associated with a substantial risk of fetal loss; Journal of the American College of Surgeons 2007; https://doi.org/10.1016/j.jamcollsurg.2007.05.025
- Oto A, Ernst RD, Ghulmiyyah LM et al.: MR imaging in the triage of pregnant patients with acute abdominal and pelvic pain; Abdominal Imaging 2009; https://doi.org/10.1007/s00261-008-9381-y
- Maralani PJ, Kapadia A, Liu G et al.: Canadian Association of Radiologists Recommendations for the Safe Use of MRI During Pregnancy; Canadian Association of Radiologists Journal 2022; https://doi.org/10.1177/08465371211015657
- Mainprize JG, Yaffe MJ, Chawla T, Glanc P: Effects of ionizing radiation exposure during pregnancy; Abdominal Radiology 2023; https://doi.org/10.1007/s00261-023-03861-w
- American College of Radiology: ACR Manual on Contrast Media. 2018; https://www.acr.org/Clinical-Resources/Clinical-Tools-and-Reference/Contrast-Manual
- British Institute of Radiology: Guidance on using shielding on patients for diagnostic radiology applications. 2020; https://www.bir.org.uk/media/414334/final_patient_shielding_guidance.pdf
17.06.2026