Guide to treat patients with myocardial bridging
A research team at Cedars-Sinai Medical Center, the University of Texas Medical Branch and RWTH Aachen University in Germany has developed a new classification system devised to guide physicians treating patients with symptomatic myocardial bridging, published in the online edition of Cardiology.
Researcher evaluated serveral diagnostic tests.
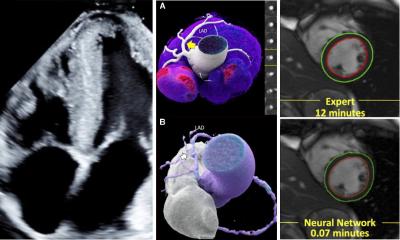
Myocardial bridging is a heart failure that occurs when the heart is malformed: a bridge of muscle fibers is overlying a section of a coronary artery, usually the left anterior descending (LAD) artery. When the heart beats, the artery is squeezed and normal blood flow is disrupted during both the pumping and relaxed cycles. This may lead to signs and symptoms similar to those caused by coronary artery disease but which are primarily the result of the entrapment and constriction of this major artery.
However, many patients show no symptoms and therefore may be unaware of their malformation unless it is detected through diagnostic imaging. Although often considered a harmless normal variant, myocardial bridging has been linked to a variety of conditions, including heart rhythm abnormalities, heart attacks and even sudden cardiac death.
“There are a number of therapies available for patients who have myocardial bridging, eg from medication management to bypass surgery. But there has been no universally accepted protocol to determine whether a requires therapy, or which option is best in each case,” said Schwarz. The study published in the online edition of cardiology evaluated the usefulness of several diagnostic tests and found out, that there are three types of patients. The international cooperation provides also guidelines for doctors choosing the most appropriate treatments for their patients.
The retrospective study included 157 patients who had myocardial bridging (MB) and no evidence of other heart disease or coronary artery disease. According to the authors, this is believed to be the largest group of MB patients in the literature and – with a five-year follow-up – the longest observation period described in the medical literature. Another 100 patients without MB, artery disease or other heart disease made up a control group.
The researchers reviewed the patients’ clinical histories for symptoms of typical angina (chest pain during stress with relief at rest); atypical angina (non-exertional chest pain); non-specific symptoms, such as palpitations and fatigue; or no symptoms. They evaluated results from non-invasive tests, such as EKGs, exercise stress tests or nuclear SPECT scans (Thallium 201 scintigraphy in single photon emission computer tomography), angiograms and invasive tests measuring different hemodynamic parameters using microtransducers within the arteries of the heart.
They found that clinical symptoms, EKGs and non-invasive stress tests are not specific for diagnosing myocardial bridging, but in patients who have myocardial bridging, clinical symptoms correlated with results from qualitative coronary angiography (QCA) and blood flow studies such as intracoronary Doppler and intravascular ultrasound.
Previous attempts to develop classification systems revolved around subjective criteria, such as the estimated percent of artery narrowing and/or the length of the compressed segment of artery.
“But they do not accurately assess arterial function. In our classification system, we incorporated clinical symptoms and results of both non-invasive and invasive diagnostic tests,” Schwarz said.
The researchers placed the 157 MB patients into three categories:
- 58 were in class A – Having clinical symptoms but no objective signs of ischemia.
- 62 were in class B – Having clinical symptoms and objective signs of ischemia by non-invasive stress tests.
- 37 were in class C – Having clinical symptoms and objective altered intracoronary hemodynamics, based on angiography and intracoronary Doppler – with or without signs of ischemia by noninvasive stress tests.
Based on initial observations and five-year follow-up, the cardiologists propose a new diagnostic work-up and therapeutic strategy:
Type A: No further diagnostic work or therapy is needed. Nitrates should be avoided. In rare cases, betablockers might be considered temporarily to relieve symptoms.
Type B: Initiate beta-blockers or calcium channel blockers. If symptoms are not relieved, quantitative coronary angioplasty or invasive blood-flow studies should be performed, after which stenting may be considered if there is objective evidence of reduced blood flow to the heart muscle.
Type C: Initiate beta-blockers or calcium channel blockers. If symptoms are refractory, consider stenting of the bridged segment.
“One of the our most important recommendations is that Type C patients – those with hemodynamic changes – always be treated, regardless of results of non-invasive stress testing,” Schwarz said, adding that the authors believe the new classification system will enable cardiologists worldwide to better riskstratify and treat patients with this frequent congenital coronary anomaly.
Photo: Siemens Med US 200711.011-03
08.07.2008
More on the subject: