Carotid artery disease
By J Larsen MD FRCR, University Department of Neuroradiology, Goettingen, Germany
Diagnostic possibilities with multi-slice CT of the neck and skull base.
However, the greatest impact of MSCT may have been on the evaluation of carotid artery disease. The vast majority of referrals for CTA certainly are in the setting of symptomatic ischaemic or haemorrhagic stroke. Applications at and below the skull base in the acute setting comprise the search for a source of arterio-arterial embolism, in particular the assessment of carotid artery stenosis, it’s site, length and degree or haemodynamic significance as well as plaque composition and documentation of possible stenosis in the proximal arterial tree which may make access to the symptomatic stenosis during secondary prophylactic procedures difficult.
The socio-economic impact of stroke disease on western societies is vast and well documented. Much work has been done to advance our ability to document in particular prognostically significant parameters that characterise carotid stenotic disease: Calcified plaque has been shown to be less symptomatic and therefore possibly more stable than a soft one. This has been confirmed by MRI studies of plaque morphology. It could be demonstrated further that the volume of calcium within carotid plaque correlates with the degree of luminal narrowing. In addition, important technical comments were made by Claves and colleagues who established that an accurate measurement of carotid stenosis depends upon the density value of the blood-contrast medium mixture as much as window settings.
Assessment of carotid stenosis
The initial evaluation of the arterial system in the neck is usually carried out using Doppler-ultrasound. This shows carotid plaque as the morphological correlate of the stenosis as well as the flow acceleration across it, which allows an estimate of its degree. However, on anatomical as well as technical grounds we require a more robust method that has, in our experience, been realised with modern CTA.
A volume scan is obtained in the caudo-cranial direction. For the assessment of the extracranial arteries, acquisition starts at the aortic arch, which allows the use of bolus-triggering software. Intracranial scans are started just below the skull base and triggered visually once contrast medium inflow is observed. In both instances scans are extended to cover the course of the callosomarginal arteries. Intracranial scans are performed with 0.5 mm collimation with no more than 1.0 mm used extracranially. From the volume data sets overlapping 0.5 mm transverse axial ‘source images’ are calculated routinely. Because of the complex image reconstruction algorithms in MSCT, consideration of manufacturers recommendations e.g. with respect to the choice of pitch etc. has been advised.
Review of the axial reconstructions alone is insufficient for the proper evaluation of a CT-angiogram. Rather a systematic step-wise image post-processing is recommended. While the patient remains on the examination table, a brief review of the source images may however be performed in order to ascertain the technical quality of the examination while gaining an overview of the gross pathology. Afterwards dedicated multiplanar reconstructions (MPR) are made on a medical imaging workstation to bring out detailed findings. Finally, 3-D reconstructions may be created for demonstration purposes only, since the degree of luminal narrowing on rendered images is highly variable depending upon window settings.
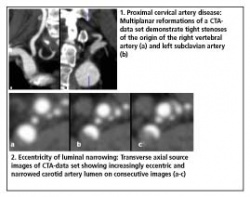
The emphasis in the evaluation of the data set is on its systematic approach. For example, demonstration of a stenosis at the origin of a proximal artery is highly relevant to the report of a skull base aneurysm if the stenosis may make access during coil embolisation difficult. Careful and systematic review of all vessels throughout their course in the source images is therefore required in the first instance. With respect to carotid stenosis, multiplanar reformations should be as thin as possible and the plane of sectioning aligned with the angulation of the course of the vessel at the point of maximum stenosis. Thin slicing is of such importance since stenoses commonly fail to assume an hourglass-like configuration but are frequently eccentric or ragged, i.e. the apparent degree of stenosis depends upon the plane of sectioning such as it depends upon the projection in conventional angiography. The minimum short axis of a luminal stenosis should therefore be measured7. In other words, maximum intensity projections are not suited to the accurate reporting of carotid stenotic disease with one exception: they are useful when choosing the length and calibre of stents prior to stent-protected percutaneous transluminal angioplasty of stenoses while serving as ‘eye-balling’-review image at the time of the procedure.
Actual measurement of carotid stenosis is carried out according to the protocols of the large international series, namely the NASCE- and ECS-trials. However, it has been shown that the so-called common carotid-method is consistently the most reproducible.
Anatomical variants and common pathologies
There are many clinically and, in particular, therapeutically relevant variants of normal arterial anatomy in the neck. These include looping and coiling of vessels. Kinking, even to a degree of significant luminal narrowing, may also occur. Such variants may be interpreted as a consequence of years of untreated arterial hypertension similar to the elongation and unfolding of the thoracic aorta. It is also recognised that the carotid artery may protrude into the sphenoid bone. The osseous membrane to the sinus may then be eroded, which is highly relevant to functional endoscopic sinus - as well as pituitary surgical procedures.
Common pathologies of carotid artery disease include aneurysms, dissection of the arterial wall and stenoses. Aneurysms may involve both the skull base or the carotid siphon. Thin MPR-images allow measurement of aneurysm dimensions relevant to the choice of the first coil for the embolisation procedure. These are equally suited to demonstrate sites and extent of dissections. Appearances of carotid stenoses vary widely. As indicated above, their site, length, degree or haemodynamic significance as well as plaque composition are relevant to the choice of possible therapeutic interventions.
* Adapted from an oral presentation, 4th Multislice CT Symposium, Charité, Berlin, August 2005
02.08.2006
More on the subject: