New perspectives in coronary plaque imaging using dual source CT
by T Henzler(1), P Apfaltrer (1), T Sueselbeck (2), D Haghi (2) , S Sudarski (1,2), M Borggrefe (1), S O Schoenberg (1), C Fink (1)
Ongoing technical developments in computed tomography (CT) such as dual source CT have established coronary CT angiography (cCTA) as a robust non-invasive imaging test for the assessment of coronary artery disease. The most important advantage of cCTA over conventional catheter-based coronary angiography is that not only the coronary lumen but also the entire coronary artery wall is visualized allowing morphologic assessment of coronary plaques.
Histopathological studies have demonstrated that myocardial infarction is caused by plaque rupture in 70% of cases and by plaque erosion in another 30%, mostly in plaques that are not associated with significant luminal stenosis. Several histopathological features that differentiate plaques with increased risk of rupture from stable coronary lesions have been identified. Non-invasive detection, characterization, and quantification of those so called “vulnerable plaques” by cCTA is desirable in order to identify “vulnerable patients” who are at high risk for myocardial infarction and to monitor the effect of drug therapy 1.
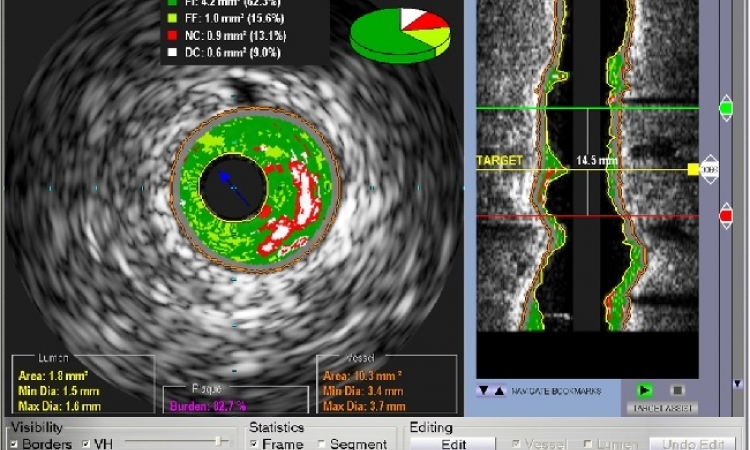
Although intravascular ultrasound (IVUS) and especially virtual histology IVUS remain the standard of reference for the characterization of coronary atherosclerotic plaques, noninvasive cCTA has shown promising advances over the past years. For adequate visualization of the coronary arterial vessel wall with cCTA, the two major technical challenges are sufficient spatial and temporal resolution. Even with CT scanners of the latest generation with a maximal spatial resolution of ~0.35 mm voxel size visualization of important plaque components of vulnerable plaques, such as the necrotic core and the fibrous cap which may measure less than 0.07 mm thickness is impossible. However, in comparison to IVUS, cCTA shows good correlation for differentiating between calcified, noncalcified and mixed plaques based on plaque attenuation measurements.
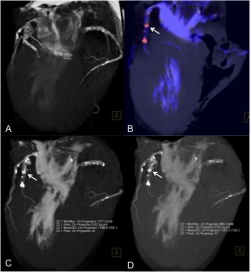
Typically attenuation values of calcified plaques range between 333 Hounsfield Units (HU) to 1944 HU, whereas noncalcified plaques show attenuation values between 26 HU and 124 HU2. This was also recently demonstrated by our own group in an ex vivo study in which plaque attenuation values were compared to the histological classification of the American Heart Association (AHA) 3. In our study Type IV plaques (atheroma) showed a mean attenuation of 11 HU whereas type Va (fibroatheroma) and type Vb (calcific) plaques showed a mean attenuation of 44 HU and 1088 HU, respectively. A limitation of all published studies that have tried to characterize coronary atherosclerotic plaques based on attenuation measurements is the large overlap of attenuation values between different types of plaques. Dual-energy (DE) CT which makes use of the two separate tube-detector systems of the dual source CT could help to overcome this limitation as different plaque types and components show different attenuation characteristics at different energy levels (e.g. 80 kV and 140 kV). This could further improve differentiation of coronary atherosclerotic plaques and reduce the overlap within attenuation values. Moreover, DECT could be used to completely eliminate calcifications in coronary arteries based on the different spectral behavior of calcium and iodinated contrast material at different energy levels.
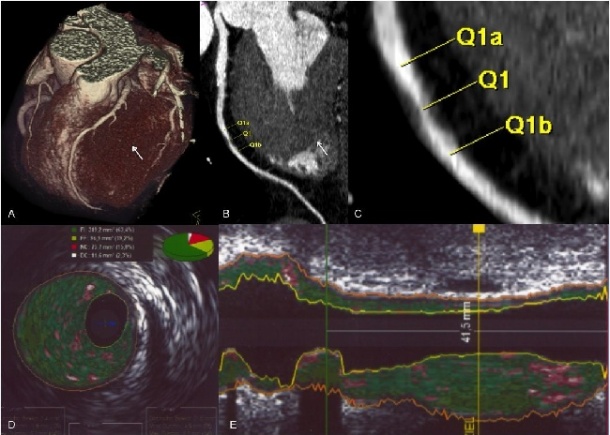
Besides attenuation based plaque characterization also advanced morphologic plaque characterization enabled by the high temporal and spatial resolution of dual source CT allow the detection of specific morphologic features indicating plaque vulnerability such as “spotty” calcifications or “rim-like” plaque enhancement 4. Further research will elucidate if non-invasive plaque characterization will improve the identification of patients with increased risk of major coronary events. In this regard we are currently performing a prospective study comparing the performance of dual source CT and DECT for the identification and characterization of culprit lesions to virtual histology IVUS in patients with stable angina pectoris and non-ST segment elevation myocardial infarction. The research is part of an international graduate college funded by the German Research Foundation.
1. Institute of Clinical Radiology and Nuclear Medicine,
2. 1st. Department of Medicine, University Medical Center Mannheim, Medical Faculty Mannheim, Heidelberg University, Germany
References
[1] Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation 2003;108(14):1664-72.
[2] Galonska M, Ducke F, Kertesz-Zborilova T, Meyer R, Guski H, Knollmann FD. Characterization of atherosclerotic plaques in human coronary arteries with 16-slice multidetector row computed tomography by analysis of attenuation profiles. Acad Radiol 2008;15(2):222-30.
[3] Henzler T, Porubsky, S, Kayed, H, Harder, N, Krissak, R, Meyer, M, Sueselbeck, S, Marx, A, Schoepf, U.J, Michaely, H.J., Schoenberg, S.O., Fink, C Attenuation-based characterization of coronary atherosclerotic plaque:
Comparison of dual source and dual energy CT with single-source CT and
histopathology. Eur J Radiol 2010.
[4] Pflederer T, Marwan M, Schepis T, et al. Characterization of culprit lesions in acute coronary syndromes using coronary dual-source CT angiography. Atherosclerosis 2010;211(2):437-44.
30.08.2010