Traumatic brain injury: The silent epidemic
Traumatic brain injury (TBI) is one of the world’s biggest public health problems. In the USA, for example, about 1.7 million people sustain TBI every year, costing healthcare $76.5 billion. Yet, the public knows little of the significance of TBI and also it once received the nickname ‘silent epidemic’ by the American
Centres for Disease Control and Prevention (CDC).

Why does this condition receive so little attention? EH reporter Karoline Laarmann asked David W Wright MD, Associate Professor of Emergency Medicine and Director of Emergency Neurosciences at Emory University School of Medicine, Atlanta, Georgia, USA, who will discuss severe brain injury in adults at ISICEM 2012.
’Traumatic brain injury is a clinical term that’s often misunderstood – because it stands for a lot of underlying damages in brain tissue,’ Dr Wright explains. ‘In general, it stands for alterations in brain function due to external force, but what it also means is that these pathologies are not visible from the outside, so that they are difficult to study or to evaluate. That’s part of the reason why it’s on the one hand so little recognised by the public and, on the other, difficult to explore in science.’
Consequently, to this day there are no medical treatments to help the brain heal after trauma. TBI treatment is limited to preventive strategies that aim to avoid further damage after the primary injury. ‘We divide TBI into primary and secondary injury,’ Dr Wright explains. ‘Primary injury occurs during the initial insult and results from displacement of the physical structures of the brain leading to contusion, concussion, etcetera. The secondary injury happens immediately after that. These are actually normal reparative mechanisms, such as haematoma and swelling, which in other body parts create no problem, but because the brain is located in an enclosed space, has devastating effects on the surrounding structures. If these processes are not controlled, the swelling herniates down through the brain stem and causes instant death.’
Therefore, clinicians today concentrate on decreasing intracranial pressure by giving infusions of hypotonic saline or mannitol, which have a substantial osmotic capacity to draw water out of the brain. In craniotomy, a surgical approach, part of the skull is removed to release pressure. Patient monitoring plays another important role, Dr Wright points out: ‘The international guidelines for the management of severe brain injury show that one episode of low blood pressure doubles mortality for patients with severe brain injury. Therefore, if you keep the vital functions up, you achieve better patient outcome. Unfortunately, these evidence-based recommendations are inconsistently followed worldwide. For instance, in the US, where the guidelines were originally developed in 1995, only 60% of clinicians follow them. That is not acceptable.’
Beyond supportive care, there is a lot of excitement about the potential of new therapeutic interventions, he reveals. ‘The brain is much more delicate than other body tissue. When you injure any other organ, or a muscle or skin, they are all made up of millions of fibres that do all the same function. Therefore, if you lose 10% of them, it is no problem – but the brain works like a computer circuit board. When you destroy 10% of the neurons, you can completely shut down critical functions. Therefore, the goal is to design treatments that stop or slow down the damage caused by secondary injury.’
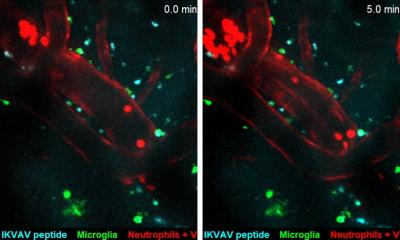
In TBI research, the greatest hope in many years is pinned on progesterone, a steroid hormone with potential neuroprotective effects. It appears to decrease brain swelling by shutting down what experts call the neurotoxic cascade. ‘Classically, this mechanism is described as shockwaves that go through the brain and release neurotransmitters like breaking the flood gates of a dam’, he explains. ‘These neurotransmitters open calcium channels that then flood into the cells and cause cell death, which then brings environmental service cells to the scene to clean up the debris. That cleaning process is what actually leads to oedema and therefore swelling. So, if we can block this linkage effect with intravenous progesterone, we probably can improve patient outcome.’
Currently underway are two Phase III clinical trials with progesterone: The ProTECT trial in the USA and the SyNAPSe study in Europe, sponsored by BHR Pharma, LLC. As principal investigator of ProTECT, Dr Wright will present the latest promising results of the trial during the ISICEM in Brussels
22.02.2012