Leading the field in PAD treatment
More procedures to treat peripheral arterial disease (PAD) are carried out in Germany than most other countries in Europe, particularly the UK, reports radiologist Dr Kai Wilhelm, from University Clinic in Bonn
Around 18,472 angioplasty procedures and 4,752 stent procedures were completed in Germany in 2008. By comparison, only 7,710 angioplasty procedures and 438 stent procedures were completed in the same year in the UK.
PAD, also referred to as peripheral vascular disease (PVD) is the hardening and narrowing of the arteries in the limbs, caused by a build up of fatty deposits (cholesterol and scar tissue) in the lining of the arteries, which reduces blood flow to the legs. PAD can be treated in a number of different ways: angioplasty (PTA) stenting or surgical intervention (bypass).
It is interesting to note that the UK lags behind other European countries when it comes to treating the femoral arteries (the most difficult to treat artery in the leg, which is often most affected by PAD), with 8,148 procedures in 2007, compared to 23,224 procedures in Germany during the same year.
PAD is quite common and affects around 6.8 million people in the UK, France, Germany, Italy and Spain. The prevalence of PAD is quite similar across all these regions, and lies between 3.83 and 4.46 percent.
The question is: Why are many more patients treated in Germany compared to, for example, the UK?
What is PAD?
PAD, also referred to as peripheral vascular disease (PVD) is the hardening and narrowing of the arteries in the limbs, caused by a build up of fatty deposits (cholesterol and scar tissue) in the lining of the arteries, which reduces blood flow to the legs.
How common is PAD?
PAD is quite common and affects around 6.8 million people in the UK, France, Germany, Italy and Spain. The prevalence of PAD is quite similar across all of these regions, and lies between 3.83 and 4.46 per cent increasing to 15 per cent to 20 per cent in persons over 70 years.
What causes PAD?
PAD is the hardening and narrowing of the arteries in the limbs, caused by a build up of fatty deposits (cholesterol and scar tissue) in the lining of the arteries, which reduces blood flow to the legs. PAD can be treated in a number of different ways: initially a conservative method of walking training and pharmaceutical intervention is advised. However, if symptoms are more advanced, with long lesions or occlusions, more invasive methods of treatment such as angioplasty (PTA) stenting or surgical interventions (bypass) become necessary.
PAD symptoms and related risk factors
Intermittent claudicatio (IC) is usually diagnosed due to a history of muscle leg pain on exercise that is relieved by a short rest. Patients with claudicatio experience reversible muscle ischemia during walking, characterised by cramping and aching in the affected muscle. These symptoms result in a severe limitation in exercise performance and walking ability. There are various risk factors for PAD. The relation between smoking and PAD was recognised in 1911. A PAD diagnosis is made approximately a decade earlier in smokers than in non-smokers. Heavy smokers have found a four-fold higher risk of developing intermittent claudicatio.
Testing for PAD
The initial clinical assessment for PAD is a history and physical examination. Palpable pedal pulses on clinical examination have a negative predictive value of over 90% that may rule out the diagnosis in many cases. The primary non-invasive PAD screening test is the ABI (Ankle-brachial Index measurement). Measuring the pressure in the ankle arteries has become a standard part of the initial evaluation of patients with suspected PAD. A reduced ABI in symptomatic patients confirms the existence of hemodynamically significant occlusive disease.
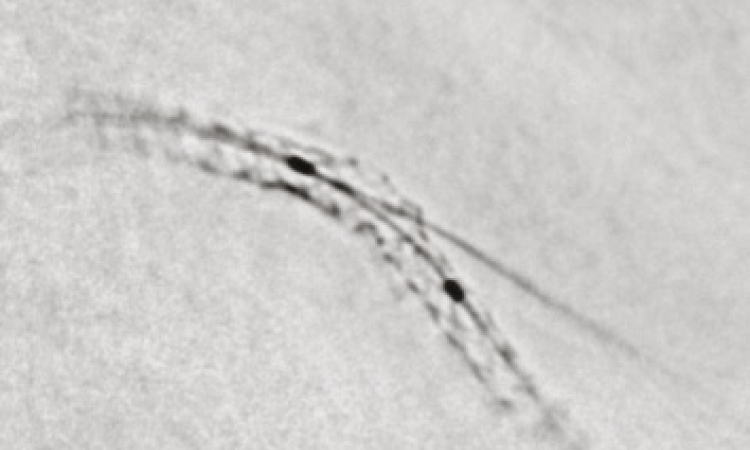
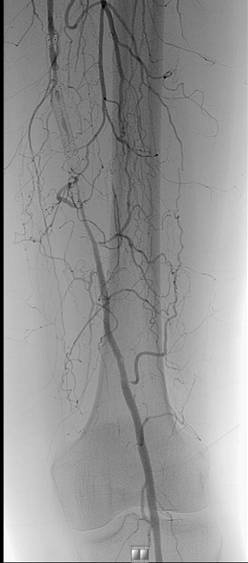
Imaging is indicated in those patients if some form of revascularisation (endovascular or open surgery) would be advised if a suitable lesion is demonstrated. Angiography, using digital subtraction technique, is considered the ‘gold standard’ imaging test and can be combined with interventional procedures such as stent implantation (see Figures). Pre-interventionally colour-assisted duplex
ultrasound is an attractive alternative, in expert hands, that can provide most of the essential anatomic plus functional information to plan an intended interventional therapy.
PAD treatment options
Patients with intermittent claudicatio, who continue to experience limitations to their quality of life after appropriate medical therapy, are candidates for revascularisation therapy. When anatomic localisation is suitable, less invasive interventional procedures are the method of choice. In the case of long-distance occlusive lesions, surgical procedures may become necessary. Why are there such huge differences in the numbers of procedures carried out across different countries within Europe? It’s probably due to a number of factors including eating habits, better diagnostic treatment of patients and earlier referral to the correct clinician.
29.12.2010