Carotid stenting: "a feeding frenzy"
Vascular experts urge caution over stent lacement to prevent stroke.
At the Vascular and Endovascular Issues, Techniques and Horizons (VEITH) Symposium) in November, attended by key opinion leaders in the field of vascular surgery, physicians remained divided on the issue of stroke prevention with carotid stent placement in patients with carotid artery disease. Most experts agree that more information is needed regarding stents, particularly for those with asymptomatic disease.
Kenneth Ouriel MD, of the Cleveland Clinic, Ohio, an avid proponent of stenting who was involved in the pivotal SAPPHIRE trial, sees a ‘big future’ for carotid stenting. ‘All the trends look in favour of stenting,’ he said in an interview.
The SAPPHIRE trial, a randomised study comparing stenting to surgery in symptomatic patients with over 70% occlusion of the carotid artery, paved the way for FDA-approval and reimbursement this year. However, it has been the subject of much debate, and the value of the study has come under heavy scrutiny by many opponents in the field of vascular surgery, who have performed the surgical procedure to remove plaque for many years with a very low risk of complications.
Carotid stenting is rapidly becoming a high-volume operation in the United States, hastened on by device-manufacturers promulgating it as a minimally invasive procedure. Frank J Veith MD, host of the symposium and Vice Chairman at the department of surgery at the Albert Einstein College of Medicine, describes it as ‘...a feeding frenzy’.
The fact that carotid stenting is generally perceived to be a lesser procedure than surgery raises the fear of implementation of widespread stenting - even in asymptomatic patients who may not be at high enough risk to justify treatment. Dr Veith shares the belief, along with other surgeons, that symptomatic patients should be treated, but that caution is warranted in implementing a stent device in asymptomatic patients.
‘I don’t know if I would go against level 1 evidence. Level 1 evidence is pretty strong,’ he stated in an interview.
‘If you leave patients with a low risk for stroke alone, then the risk of getting a stroke per year is about 1.5%, which is low,’ said Peter R F Bell MD, a vascular surgeon at the Leicester Royal Infirmary in the United Kingdom, and leading opponent to the SAPPHIRE trial. In Europe there is the tendency not to operate on low risk patients, while in the US, historically, such patients have been operated on, he explained. ‘A 3% risk for stroke and death has been established as the acceptable rate of complications associated with surgical treatment,’ he pointed out, referring to results from the recent European ACST trial. ‘There has never been a good study showing that carotid stenting reduces stroke rate to that level,’ Dr Veith added.
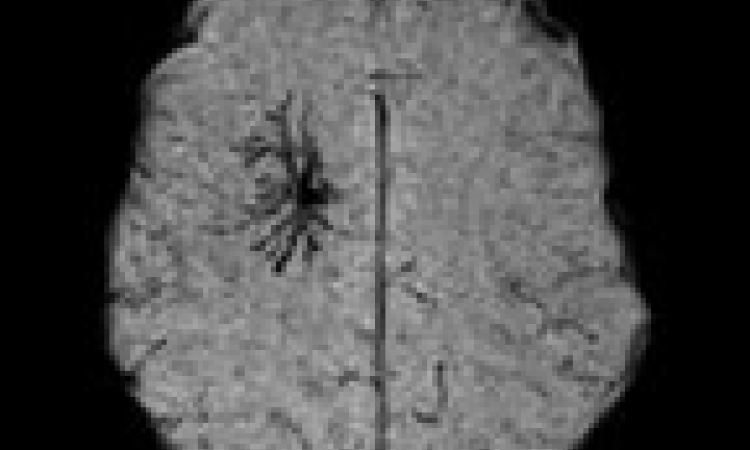
The industry’s apparent push to replace it by a procedure that remains yet to be proven in prospective, randomised trials, has many stroke experts alarmed, particularly since the procedure is not without inherent risks, such as embolisation to the brain, a complication affecting up to 80% of patients.
In a scathing rebuttal to Dr Ouriel’s defence of SAPPHIRE at the symposium, Dr Bell contended that SAPPHIRE was industry-funded and its investigators lacking in equipoise-’It is just not the trial on which you should base a whole trend of treatment, which is what they are suggesting.’
A recent Cochrane systematic review found insufficient evidence to support widespread change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis. ‘It is ethical and necessary that randomised trials comparing endovascular treatment with surgery continue to recruit patients,’ authors concluded.
Most experts at the symposium agreed that patient selection for intervention remains crucial, since inappropriate selection of patients or poor surgery could obviate any benefits.
The potential problem of over-treatment looms large. ‘Invasive treatment should not be given where it causes more trouble than it’s worth,’ Dr Bell said.
Invoking the conscience of physicians and their professional ethos, and in a critique of the SAPPHIRE trial, Dr Bell declared at the symposium, ‘It is our duty as physicians to protect our patients from these risks and do a proper trial that actually tells us what’s the right thing to do. The only person who actually is responsible for what happens to the patient is you, the doctor. The industry doesn’t care, the government doesn’t care - nobody cares apart from the doctor.’
Well, what about the patient? The patient foremost needs to understand and become knowledgeable about the risks and benefits related to both stenting and surgery, which will hopefully emerge with greater clarity as more data is revealed from ongoing trials.
ACST and ACAS trials cut the 5-year stroke risk in half with very low peri-operative morbidity. These trials showed that you can treat asymptomatic disease with a stroke and death rate of around
2-3%. ‘That’s the ball park,’ said Peter A Schneider, Managing Director of the Hawaii Permanente Medical Group, speaking at the symposium. ‘You’ve got to be in the ball park to have something that I think will be of value to the patient.’
In the end, it all depends on how the risks and benefits are phrased by the doctor to the patient. ‘If you tell them, look, I have something that is going to work 95 percent of the time, they’ll say they want it. And that can be a stent at this point. It has that kind of success rate,’ Peter Schneider explained. ‘But if, on the other hand, you say you can have a stent, but the risk of stroke or death is going to be twice as high, they’ll say ‘I’d rather have the surgery’. So it all depends on how you present the data to them.’
Stenting proponent Dr Ouriel acknowledges that SAPPHIRE did not show superiority of stenting over surgery, but ‘did show non-inferiority.’ He stated in an interview, ‘...it doesn’t show we shouldn’t be choosing endarterectomy in these [high risk] patients, but it does say we should consider stenting and we certainly should be offering that to the patients as a viable option. I personally try to give my patients that data and most of them will pick stenting - almost all - will pick stenting over endarterectomy.’
23.05.2006