

Work analysis
The problem is ubiquitous: Due to their workload, medical teams cannot accomplish their tasks to everyone’s satisfaction during regular working hours. Is the solution to raise staffing levels? More politics? At a political level a framework could be created but its actual implementation must occur within a facility, because that is where work schedules are drawn up, writes Denise Hennig, reporting on a work analysis system produced by Documix GmbH, of Grebenhain- Bermutshain, Germany. The system, available in the German language, is currently utilised at the Katholische St Johannes Gesellschaft, Dortmund (comprising four hospitals), Karl Olga Hospital, Stuttgart, and the Lungenklinik Hemer.
Improving patient care, job satisfaction and personnel costs
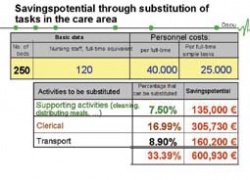
Medical personnel may perform several tasks that lie outside their professional scope, which, quite often, could be performed more cost-effectively by other employees. Nurses, for example, might become involved in cleaning, food distribution, clerical work and transportation, whilst doctors might take on wound and/or patient management and administration. Using overqualified staff for these tasks is not only a significant waste of resources (see table) and finance, but could also demotivate physicians or nurses who must undertake activities unrelated to their professions. Providing more appropriate personnel for those activities could alleviate the problem.
The solution lies in reporting and work analysis. Traditional procedures, such as self-reporting or multi-moment analyses, provide only marginally useful results if medical or nursing activities last only four to eight minutes. The answer lies in data capture on mobile digital equipment, such as the Documix DocuLine. About the size of a pocket calculator (14 x 7 x 1.5 cm) this device has a keypad, display and integrated bar code scanner.
During their shifts, staff members use the device to enter all services provided to each patient. The software ‘DocuKeeper’ transmits this data to the ward computer, which contains the entire data management, e.g. patient records, etc. A further programme, DocuAnalyst, analyses the services data, and the results suggest where changes and adjustments to work structures could be useful.
The percentage of activities not directly related to professional qualifications varies from profession to profession. The analysis can show not only which activities are often interrupted due to external demands on a staff member, but also illustrates the interdependence of the various groups. On some wards, for example, the permanent presence of nurses during visiting times could create problems if not enough staff is available to tend patients in need.
Peak times and off-peak times
Certain activities are sometimes performed too quickly, simply due to the workload, whilst during quieter periods tasks can be performed with full concentration. A constant swing from extreme peaks to off-peaks and back creates additional and avoidable staff stress.
Once reliable measurements of workflow and durations are obtained, the staff should discuss those facts, together, to make realistic work allocations. The degree to which these have been adopted can be assessed during follow-up measurements. An important side effect is that costs can also be assessed.
It is a hospital’s task to make and implement the necessary decisions. Adjusting the workforce structure is a more sensible solution than making staff redundant, and it is a solution from which, in the end, everyone will benefit:
• Physicians and nurses are relieved from non-profession-related activities
• The hospital will save on personnel costs
• Patients will be better cared for because medical staff can focus on core tasks.
Additional benefits: improved documentation, precisely calculable personnel costs for individual DRGs, or empirically supported patient paths that will be useful to other departments. Using the analysis, the PPR (Pflege-Personalregelung) regulation regarding care personnel requirements) or LEP (Leistungserfassung für die Pflege) reporting of care services data can be verified.
However, the most important issue is not the technology (even the most sophisticated data collection will end up in the bin if results are not implemented) but the will and capacity of a hospital to manage change.
Details: www.documix.de
01.03.2006


