

Source: Unsplash/Kyle Glenn
Article • Detecting migrant health risks
‘Refugees do not bring diseases to western shores’
The migrant population is fast growing and heterogeneous. Experts at a session held during the European Congress of Radiology (ECR 2019) concluded that radiologists can play a key role in detecting and differentiating related diseases.
Report: Mélisande Rouger

Migration is a growing phenomenon and has an impact on health, according to Jozef Bartovic from the World Health Organisation (WHO) in Copenhagen, Denmark. ‘We’ve seen a huge increase in migration over the last few decades, and about 10% of global population today are international migrants. There is a huge heterogeneity of resources, backgrounds, exposure to risks, which are all important to consider in healthcare. Refugees are just 7% of all migrants,’ he said.
Key migration factors can lead to health problems before, during and after migration. War impacts on mental health before and after migration. Violence during migration, for instance smuggling, burns or drowning, has consequences on a migrant’s health. Discrimination and low levels of integration in the host country can also trigger health problems.
The WHO refugees and migrants’ health in Europe report states: Migrants do not bring diseases with them to their country of destination. ‘Refugees and migrants are generally in good health, but can be at risk of falling ill during the transit period and in the receiving countries, due to poor living conditions and adjustment to their new lifestyle,’ Bartovic pointed out.
Considering the incubation period of most bacterial and viral infections, most migrants will be either cured or dead by the time they arrive in the destination country. Living in a refugee camp, for instance, can provoke a number of diseases that can be fatal and take up considerable healthcare funds if untreated. Very early detection and correct treatment of diseases is key. ‘The links between migration and radiology are worth exploring, especially regarding access to services, legal barriers, health service capacity and continuity of care,’ he said.
Recommended article
Article • Combatting infections
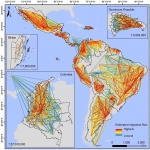
The global migration mapping project
Experts at a university in the United Kingdom have designed a large-scale data and mapping project that they hope will help in the global fight against infectious diseases.
TB or not TB

The most common migration diseases relevant to radiology are pulmonary and extrapulmonary tuberculosis (TB), according to Tim Weber, senior physician at the Institute of Diagnostic and Interventional Radiology in Heidelberg. ‘TB is the most common infectious disease in the migrant population. There’s a difference between TB in the migrant population, which affects mainly young people, and TB in the host population, where it’s typically a disease of the elderly.’
The main challenge for radiologists in pulmonary TB is to differentiate between active and inactive TB. Active TB typically presents as consolidations with cavitations and formation of centrilobular nodules due to bronchiolitis after bronchogenic spread of microbacteria. Necrotising adenopathy and pleural effusion are further signs that should alert the radiologist. Inactive TB is characterised by fibronodular scarring, volume loss and calcifications. An important feature in ambiguous cases is stability of imaging findings over time, so follow-up is recommended.
Pulmonary TB is atypical in HIV+ patients; especially in patients with CD4 lympho count <20/nm typical features of TB. ‘Typical features of TB like cavitation or adenopathy are lacking, and other unspecific consolidations are primary imaging findings,’ Weber said. Rapid diagnosis in this fragile population is important. also of note: TB risk is 20 times higher in HIV + patients.
Most radiologists know that extrapulmonary TB can affect any organ, because haematogenous spread of microbacteria is almost always present during primary TB. Extrapulmonary TB can be abscess forming, but can also present with soft tissue infiltration. ‘This is also a reason why extrapulmonary TB is known as the great imitator, mimicking a variety of infections and neoplastic diseases,’ Weber explained.
Sometimes no imaging findings can help distinguish between intestinal TB – TB ileum – and Crohn’s disease. One can detect fistula and chronic inflammation, e.g. proliferation of mesentery fat, possibly present in both diseases. In pulmonary TB, the main task is to differentiate between active vs. inactive TB, and consider TB in any pulmonary infiltrate.‘Extrapulmonary tuber- culosis should be considered in any suggested inflammatory or neoplastic disorder,’’ he advised
Worm-caused diseases
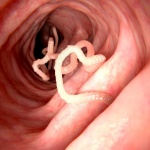
Cystic echinococcosis (CE) and schistosomiasis are two other common conditions that mainly affect migrants. CE is caused by dog tapeworm and has a global distribution. Almost eradicated in most western industrial countries, there is only scarce data on prevalence in migrants - however, CE will be diagnosed in a large number of refugees or migrants. CE causes cystic expansive mass, which can grow in any part of the body, mostly the liver or the lung. Serology test can be negative in a number of patients and imaging is essential for diagnosis. CE shows with specific pathognomonic signs on imaging, such as the water-lily sign (CE 1), the rosette sign (CE 2), the Swiss cheese sign (CE 3b) and the ball of wood (CE 4). ‘The major CE feature is that there is complete absence of vascularity, thus contrast imaging studies should be performed to exclude neoplasm,’ Weber said.
Recommended article
News • Experts' discussion
How to tackle parasitic worms
Parasitic worm infections – or helminthiases – affect more than one billion people and have a considerable public health impact in many parts of the world. In December 2017, international experts gather in Basel, Switzerland, to discuss new strategies to control and eliminate parasitic worms. The scientific symposium is hosted by the Swiss Tropical and Public Health Institute. Approximately…
Schistosomiasis, a set of diseases caused by trematode worms, or blood flukes, is very common in tropical and subtropical regions; more than 150 million people are affected in sub-Saharan Africa alone. The worms produce eggs that are embolised via the portal vein to the liver, inducing chronic liver inflammation, which can lead to periportal hepatic fibrosis or Symmer’s pipe stem fibrosis. Here also, imaging can help, notably to differentiate between liver cirrhosis and schistosomiasis.
Profiles:
Technical officer Jozef Bartovic at WHO/Euro, contributes to the PHAME project, the Knowledge Hub and the Migration and Health Knowledge Management Project. Previously, working for the Regional Commission for Western Asia of the UN Secretariat in Beirut, Lebanon, he covered migration and displacement issues in the Arab region. Originally from Slovakia, after completing political studies he worked in the UK for the Ministry of Health, Public Health England (Health Protection Agency) and the NHS on screening programs, sexual and reproductive health and primary care access.
Tim Weber MD is a senior physician at the Institute of Diagnostic and Interventional Radiology, in Heidelberg University Hospital, Germany.
17.06.2019


