CT is still the be all and end all
At this year’s meeting of the German Radiological Society (DRK), Dr Mathias Langer, Head of the Radiology Clinic at Freiburg University Hospital and the society’s 2013 President, assured EH that CT is still the be all and end all in trauma surgery.
‘As yet,’ he explained, ‘there is no alternative for the care of acutely injured patients, and there’s a simple reason for this. Taking conventional X-ray images is considerably more time-consuming then CT. Also, modern CT systems are now so good that radiation exposure is almost no issue at all these days…’
… although this procedure was also being performed before this was the case.
‘Yes. And the third reason, which also explains why this procedure was being used before, is the type and amount of information it delivers about patients that cannot be obtained with conventional radiology.
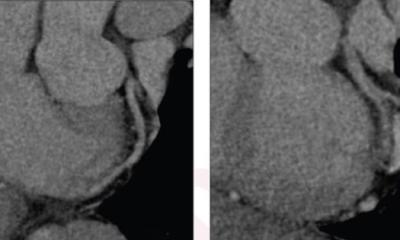
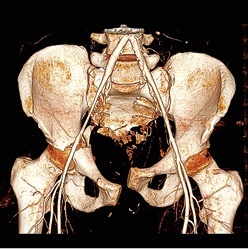
This starts with the classic diagnosis of epidural or subdural haematoma, assessed with the help of CT for the last 20 years, and extends to vascular lesions in the thorax and abdomen/pelvis, injuries to the liver and spleen, as well as spinal injuries such as vertebral fractures, which, during repositioning of a patient, can potentially cause paraplegia. CT with contrast agents provides a clear diagnosis for arterial or venous injuries in the pelvic area or the legs so that, for example, imminent haemorrhagic shock from a pelvic fracture can be detected. Radiological intervention can then quickly help the patient.’
What are the current drivers in this field if there are no technological challenges?
‘To say that there are “no technological challenges” would be an exaggeration. A topical point at the moment is the immediate integration of the CT unit with the A&E department – in other words, a reduction in the amount of time wasted due to long distances between the resuscitation room and CT. Furthermore, there are still many systems in clinical use that do not meet current demands in this highly technological field, i.e. the initial and immediate diagnosis of bones, soft tissues and the entire vascular system in just one examination taking less than half a minute for data acquisition.’
Down to the awkward question of money, is that correct?
‘Yes, of course.’
How can you manage without a system that can do all this in under a minute?
‘With good anaesthesia, good patient monitoring and optimal timing of the various examinations, i.e. with excellent interdisciplinary cooperation based on standard operating procedures jointly established by the team. This ensures that the patient can be monitored and cared for in the best possible way, and that a timely diagnosis is achieved despite longer examination times. Without good organisation even the most up to date technology does not really help.’
07.08.2014