News • Health economics
Atrial fibrillation imposes a high burden in Europe
The first health economics data from the Global Anticoagulant Registry in the Field – Atrial Fibrillation (GARFIELD-AF) was presented at ESC Congress 2017, organised by the European Society of Cardiology, in Barcelona, Spain.
These data demonstrate that AF imposes a high financial, economic and human burden on societies across Europe and that there is significant geographical variation in the amount and type of health services used by patients across the world.
In a poster presentation entitled “The burden of atrial fibrillation in the more populated European countries: perspectives from the GARFIELD-AF registry”,1 data were presented on patients with AF enrolled in France, Germany, Italy, Spain and the UK during 2010–2015. These patients generated a total of 8,574 person-years (pys) of observation. Large variations among the five countries were seen, with higher costs per patient per year in the UK (£2,857.3) and Germany (€2,504.1) than in the other countries. Direct costs in each country also differed in the type of costs, with outpatient care as a proportion of the total cost ranging from 9.4% in Italy to 25.1% in Spain. Expenditure for hospital admissions also varied, from 63.9% of the total cost in Spain to 83.7% of the total cost in Italy.
The authors concluded that the great variations observed in the cost for drug treatment can probably be ascribed to different combinations of treatment. Additionally, based on population dynamics, the current financial, economic and human burden of AF is likely to grow in the future. Furthermore, premature mortality substantially adds to the already considerable direct cost of the disease.

In a second health economics poster entitled “Global healthcare resource use in 39,670 patients with AF: perspectives from GARFIELD-AF”,2 data from patients with AF in 35 countries were analysed. Enrolled patients together generated 30,117 pys of observation (Asia 7,521; Europe 18,358; Latin America 2,630; North America 780; rest of the world 827). A total of 402.3 medical contacts per 100 pys were documented overall, corresponding to an average of more than 4 medical contacts (any type) per patient per year. North America and Europe showed higher healthcare resource utilisation (HCRU) (544 and 432 medical contacts per 100 pys, respectively) than Asia and Latin America (344 and 360 medical contacts per 100 pys, respectively).
Of the vast amount of healthcare resource utilised worldwide, there were significant geographical variations in the amount and type of health services used by patients which, the authors concluded, were potentially associated with the actual availability of services and different models of care organisation in the 35 countries.
The lead author of the two posters, Professor Lorenzo G Mantovani, Associate Professor of Public Health, University of Milan Bicocca, Monza, Italy, commented: “The variability observed in cost items among the five European countries is mostly likely driven by healthcare reimbursement practices and not by inherent differences in patients’ status or type of treatment. Improving outcomes in younger patients would have a great impact in terms of burden to societies.”
He continued: “Furthermore, in terms of HCRU, the next step is to link clinical outcomes of patients with AF among different regions in order to understand the cost-effectiveness of different patient management strategies and to identify the most beneficial approach.”

Earlier during the Congress, at the dedicated Thrombosis Research Institute (TRI)-sponsored Satellite Symposium, members of the GARFIELD-AF registry Steering Committee outlined the real-world outcomes over 1 year after diagnosis of AF in all 52,081 patients prospectively recruited into the GARFIELD-AF registry. In his opening remarks, Professor the Lord Ajay K Kakkar, Director of the TRI, London, UK, explained that the learning objectives for the symposium were to:
- understand how comorbidities impact the prognosis of patients with AF
- appreciate the importance of comprehensive management of AF
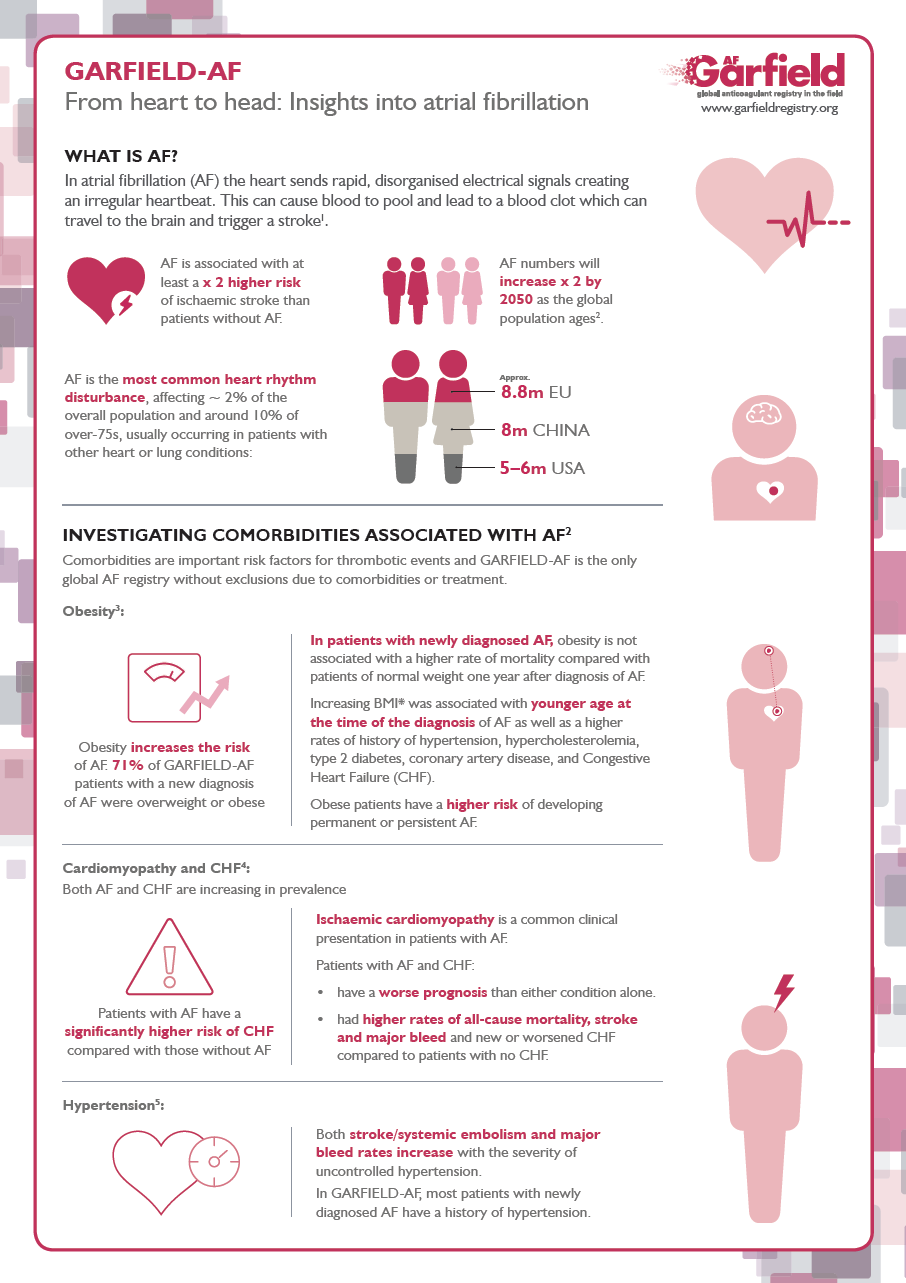
Examining the burden of AF, specifically in regard to morbidity and mortality, Professor Samuel Z Goldhaber, of Brigham and Women’s Hospital and Harvard Medical School, Boston, USA, concluded that AF is a risk marker for systemic disease and a risk factor for stroke. The first mission for clinicians in patients with AF is to prevent stroke. He explained that the data showed heart failure was a common cause of death, and that elevations of d-dimer, troponin, and brain natriuretic peptide (BNP) were also predictive of stroke. While the rate of anticoagulation appeared to be similar in women and men in GARFIELD-AF, for unknown reasons women had a higher risk of stroke/systemic embolism (SE) than men. “This highlights the requirement for patient involvement and empowerment, educational guidance and shared decision-making in integrated AF care,” he said.
High rates of comorbidities were found in GARFIELD-AF, including congestive heart failure (CHF) 20.6%; history of coronary artery disease 19.9%; history of acute coronary syndrome (ACS) 9.4%; history of hypertension 77.5%; overweight/obese 71.0%; diabetes mellitus 21.7% and moderate-to-severe chronic kidney disease (CKD) 10.4%.
The major contributors to adverse outcomes in patients with AF and prior ACS are cardiovascular death and new ACS
Keith A A Fox
In his presentation, Professor Alexander G G Turpie, of McMaster University, Hamilton, Canada, focused on the profile and outcomes of patients with AF and congestive heart failure. He noted that 18% of patients with newly diagnosed AF presented with CHF, and that these patients were older/sicker than those without CHF. Anticoagulation was similar between groups, but the sicker patients (denoted as New York Heart Association [NYHA] class IV) were more likely to receive antiplatelet (AP) therapy. Although there was better implementation of recommended CHF treatments in NYHA class III/IV patients, particularly aldosterone blockade, prescribing of digitalis drugs remained high. Overall, the burden of cardiovascular morbidity and mortality increased markedly with NYHA class. While patients with NYHA class I seemed to have similar outcomes to patients without CHF, they suffered from a higher rate of worsening CHF over the year after the diagnosis of AF.
Professor Keith A A Fox, of University of Edinburgh, Edinburgh, UK, spoke about management and outcomes in acute coronary syndromes with AF, asking where things can improve. He explained that event rates after ACS, especially with AF, increase over time, noting bleeding rates were low if patients were on oral anticoagulants (OACs) without AP therapy. However, perceived bleeding risk was a frequent reason for not using OACs. In patients with AF and prior ACS, patients are increasingly on combined AP and AC therapy – and this combined antithrombotic therapy is associated with a modest increase in bleeding. “The major contributors to adverse outcomes in patients with AF and prior ACS are cardiovascular death and new ACS,” said Professor Fox.
Geographic differences in the routine care of patients with chronic kidney disease and AF were examined by Professor Shinya Goto, of Tokai University School of Medicine, Kanagawa, Japan. He said that of patients with newly diagnosed AF, 16% have mild CKD and 10% moderate-to-severe CKD. Advanced CKD stage was also associated with a higher rate of other comorbidities. “Surprisingly”, he said, “the use of OACs in patients with AF was similar across the stages of CKD even though patients with moderate-to-severe CKD demonstrated a higher risk of stroke/SE, serious bleeding and mortality than those with no CKD. Similar trends were shown in most regions for the three endpoints.”
Examining the impact of body mass index (BMI) and the metabolic syndrome on AF outcomes, Professor A John Camm, of St. George’s University of London, London, UK, said that the majority of patients with newly diagnosed AF were overweight or obese. Patients with morbid obesity (and associated metabolic syndrome) were almost 10 years younger (median) than patients of normal weight when diagnosed with AF. Furthermore, higher BMI was associated with greater use of anticoagulants. Overall, underweight patients have a higher risk of death (vs normal weight patients) 1 year after AF diagnosis. Professor Camm concluded that as BMI increased, mortality paradoxically decreased in GARFIELD-AF – although this effect may be reduced after adjustment for baseline characteristics such as age.
In his concluding remarks, Professor Jean-Pierre Bassand, of University of Besançon, Besançon, France remarked on the striking changes in the patterns of anticoagulation from GARFIELD-AF cohorts 1 to 5, with the rate of anticoagulation increasing from 57.4% to 71.2% and uptake of non-vitamin K antagonist oral anticoagulants rising from 4.2% to 43.1%.
Professor Bassand also commented on causes of mortality, confirming that death was the most frequent adverse event in AF and occurred at a three-fold higher rate than stroke/SE and a five-fold higher rate than major bleeding. Similar rates of cardiovascular and non-cardiovascular death were observed. CHF, malignancy, infection/sepsis, respiratory failure and sudden death were the most frequent known causes of death, with stroke being accountable for only 5.5% of all known causes of death.
Regarding comorbidities, Professor Bassand said that the rate of anticoagulation was suboptimal in the sickest patients, irrespective of the comorbidity under consideration. In addition, more than two-thirds of patients received no OAC treatment after 4 months. Moreover, the comorbidities associated with worse outcomes in patients with AF, namely CHF, vascular disease and CKD, were suboptimally treated in around 50% of the cases.
To view the seven GARFIELD-AF posters presented at the ESC Congress 2017 and a video recording of the TRI Satellite Symposium, please log on to the GARFIELD-AF website at: www.garfieldregistry.org/.
Source: GARFIELD-AF
30.08.2017