Trends in cardiac pacing
The cardiac pacemaker of the future will be wireless and monitored by the physician via satellite, says EH writer Holger Zorn
‘Sacrilegious meddling with divine providence’ was the charge brought against New York cardiologist Alfred Hyman in the 1930s when, after successful animal experiments, he applied the first cardiac pacemaker – then still a cumbersome external device – in human patients. A quarter of a century later the first cardiac pacemaker, mounted in a shoe polish tin and covered by epoxy resin, was implanted. However, Swedish heart surgeon Ake Senning, of the Karolinska Institute, and engineer Rune Elmqist of Siemens-Elema, were not confident that their development, which had worked for a mere three hours, would become a medical success. Unlike the inventors, the patient, Arne Larsson, believed in the new device and underwent more than two dozen implantations.
Courtesy of Dr Christian Butter, Herzzentrum Brandenburg.
Small device, big business
In 2008, the year that marked the 50th anniversary of the first pacemaker implant, Sreevidhya Praveen, analyst for consultants Frost & Sullivan, determined a market volume for pacers of €2.68 billion in Western Europe alone. For 2015, Praveen predicts the business will reach €5.76 billion. Three drives currently propel pacing technology: cardiac resynchronisation therapy (CRT), telemonitoring and – newest of all – wireless pacing.
CRT
In 1994, Serge Cazeau of the Institut Parisien de Rythmologie et de Stimulation Cardiaque (InParys) presented CRT, a device that improves the heart’s pump function in patients with congestive heart failure (CHF). This progressive cardiac disease, which in advanced stages may require major interventions such as a heart transplant, usually entails a gradual loss of heart muscle. The remaining tissue cannot transmit the electrical impulses. The CRT device contains three rather than the usual two leads, which are fastened to the wall of the heart – in the right atrium and the left and the right ventricle. By pacing both chambers the heart beat is coordinated – resynchronised.
Several studies indicate dramatic benefits of CRT. According to the Multisite Stimulation in Cardiomyopathies (MUSTIC) trial, CRT reduced the number of hospitalisations by two thirds [Source: Europace 2004;5:42-8]. This has a significant impact not only on patients’ quality of life but also on healthcare costs: With a prevalence of 2–2.5%, around 15 million people in Europe suffer from CHF; about 400,000 new cases per year will be recorded.
Frieder Braunschweig of Karolinska Hospital analysed 16 patients who received CRT. He found that the number of hospital days decreased from 253 days in the year before the CRT device had been implanted to 43 days in the year after the implant (p<0.01). Average total costs of in-patient care per patient were €9,301 per pre-implant year and €1,654 in the year following the implant. With average implant-related costs of €8,019 per patient, CRT had paid off in the second year [Source: Eur J Heart Fail 2000;2:399-406].
Wireless pacing
Frequently, the usual access route to place the third lead – the coronary sinus – is blocked. WiCS, wireless cardiac stimulation technology developed by EBR Systems Inc., Sunnyvale, California, offers a way out. The device is co-implanted with a conventional CRT system since ‘the leads have always been the weakest link in any cardiac pacing system,’ explains Dr Debra Echt, co-founder of EBR Systems. Dislodgement and failure due to fatigue occur in about every fifth lead.
In the course of a feasibility and safety trial Dr Christian Butter, Head of Cardiology at the Heart Centre Brandenburg in Bernau, Germany, recently implanted three of the currently six devices in use worldwide.
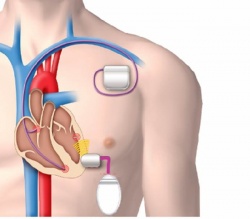
He inserted a wireless receiver/transducer via catheter through the femoral artery, the aorta and the aortic valve in the left ventricle and fastened it to the posterolateral ventricle wall. The generator is implanted on the left side below the sixth rib, about eight centimetres away from the lead. Upon sensing the stimulation of the right ventricle by the CRT device, the generator transmits its own pacing impulse using a frequency of 800 kHz to the receiver in the left ventricle (Fig. 1).
If the device were implanted at the usual location below the sternum, the lungs would absorb and the ribs would curve and break the sound waves. With the new device, Butter explains, ‘different sites in the left ventricle can be stimulated independently of the venous anatomy. Implantation of a wireless lead makes CRT an option for many more patients.’
The technology allows access to further pacing sites in the right ventricle or the right atrium and it can replace all pacing leads – maybe even all sensor leads. Continuing along these lines, Butter is convinced, will one day provide a device in which the entire technology is set in a single housing and uses several frequencies. This will be the advent of fully wireless cardiac pacing.
Fully wireless pacing is by no means science fiction, as N Oesterle MD, Vice President for Medicine and Technology at Medtronic, showed at TEDMED, held last October in San Diego: The next generation cardiac pacemaker will be inserted via catheter through the blood vessels, the right ventricle and the septum into the left chamber. There, right at the pacing site, the device will be fastened to the ventricle wall with four hooks. These hooks – and this is the most amazing idea behind the technology – serve as leads (Fig. 2). Oesterle expects this technology to reach marketability in three to four years.
Telemonitoring
Technology can indeed develop from science fiction to clinical reality in just a few years – as telemonitoring shows. Today, data are transmitted from a pacemaker, implantable cardioverter/defibrillator (ICD), or CRT device to an internet-based platform from where they can be retrieved by the physician.
Biotronik Home Monitoring by Biotronik SE & Co. KG Berlin handles this communication wireless, automatically and safely via the frequency range reserved for medical implants (403 MHz) and the mobile phone network. Technical and clinical data are regularly coded and transmitted to the Biotronik computer centre where they are decoded, analysed and summarised in reports that the physician in charge can access via internet (Fig. 3). Clinically relevant data are transmitted instantaneously and the physician is alerted via text message, e-mail or fax. This not only improves early detection and allows timely intervention by the physician but also reduces the number of visits at the physician’s office.
In the TRUST Landmark study Niraj Varma et al. of Cleveland Clinic, Ohio, compared 473 ICD patients who received conventional follow-up – out-patient presentation after 3, 6, 9, 12 and 15 months – with 977 patients who presented only twice – after three and 15 months – for follow-up and underwent Biotronik Home Monitoring (and were called in as required). This procedure decreased the number of hospitalisations by 45% within one year – while maintaining utmost patient safety.
Furthermore, the study showed that arrhythmias are detected much earlier: The time between a recorded event and its analysis by a physician occurred on average in less than two days compared to 36 days in the control group [Source: Circulation 2010;122:325-32].
Cardiac contractility modulation (CCM) is an upcoming method to treat cardiac insufficiency of those patients who do not or no longer benefit from cardiac resynchronisation therapy – which applies to at least 30% of them [Source: Eur J Heart Fail 2007;9:955–8].
In contrast to conventional cardiac pacing, CCM signals do not initiate a heartbeat. In contrast to cardiac resynchronisation therapy, CCM do not alter the activation sequence. Instead, CCM signals are delivered after a preset delay following detection of muscle activation. This augments the calcium influx into the heart muscle cell – and calcium is essential for cardiac contractility. The effect is an improved ejection fraction, thus an improved exercise capacity, measured by peak oxygen consumption, and a better quality of life.
Moreover, Christian Butter, head of cardiology at Brandenburg Heart Centre and one of the pioneering investigators of CCM, confirms ‘there is no adverse effect on long-term survival’.
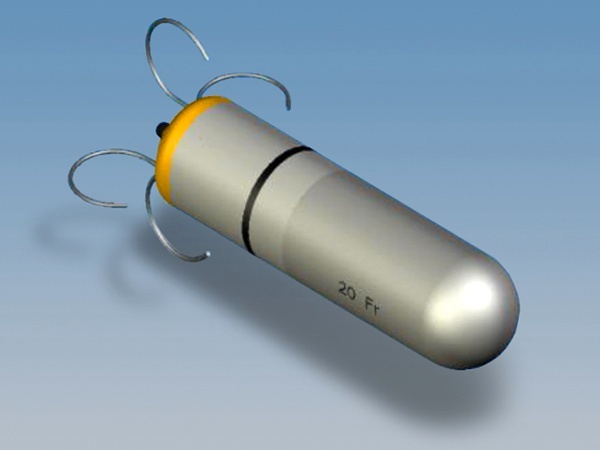
He recently reported 59 consecutive patients who underwent CCM therapy [Source: Europace 2011 Jun 28; Epub ahead of print] with implantation of an Optimiser system from Impulse Dynamics, presently the only manufacturer of such a device (pic. 1).
Since its clinical introduction, there are more than 750 patients treated with CCM in Europe. Germany, often berated for restrictive reimbursement of innovative therapies, has included this therapy in its DRG system: With a cost weight of 9.018, and depending on their base rate, hospitals earn about €27,000.
26.08.2011