

All photographs courtesy of Dr Yann Nguyen / Collin Medical SA
Article • Robotic assistance for middle and inner ear procedures
Cochlear implant microsurgery progresses
Unlike other surgical specialties, ear nose and throat (ENT) has been poorly served by the introduction of robotic platforms to enhance procedures. Since the da Vinci system first gained FDA approval in 2000, robot-assisted surgery has become commonplace in many specialties, including neurology, urology, etc. with numerous other general surgical applications. However, existing systems including the da Vinci are not easily exploitable for the microsurgical techniques used in inner and middle ear procedures.
Report: Jane MacDougall
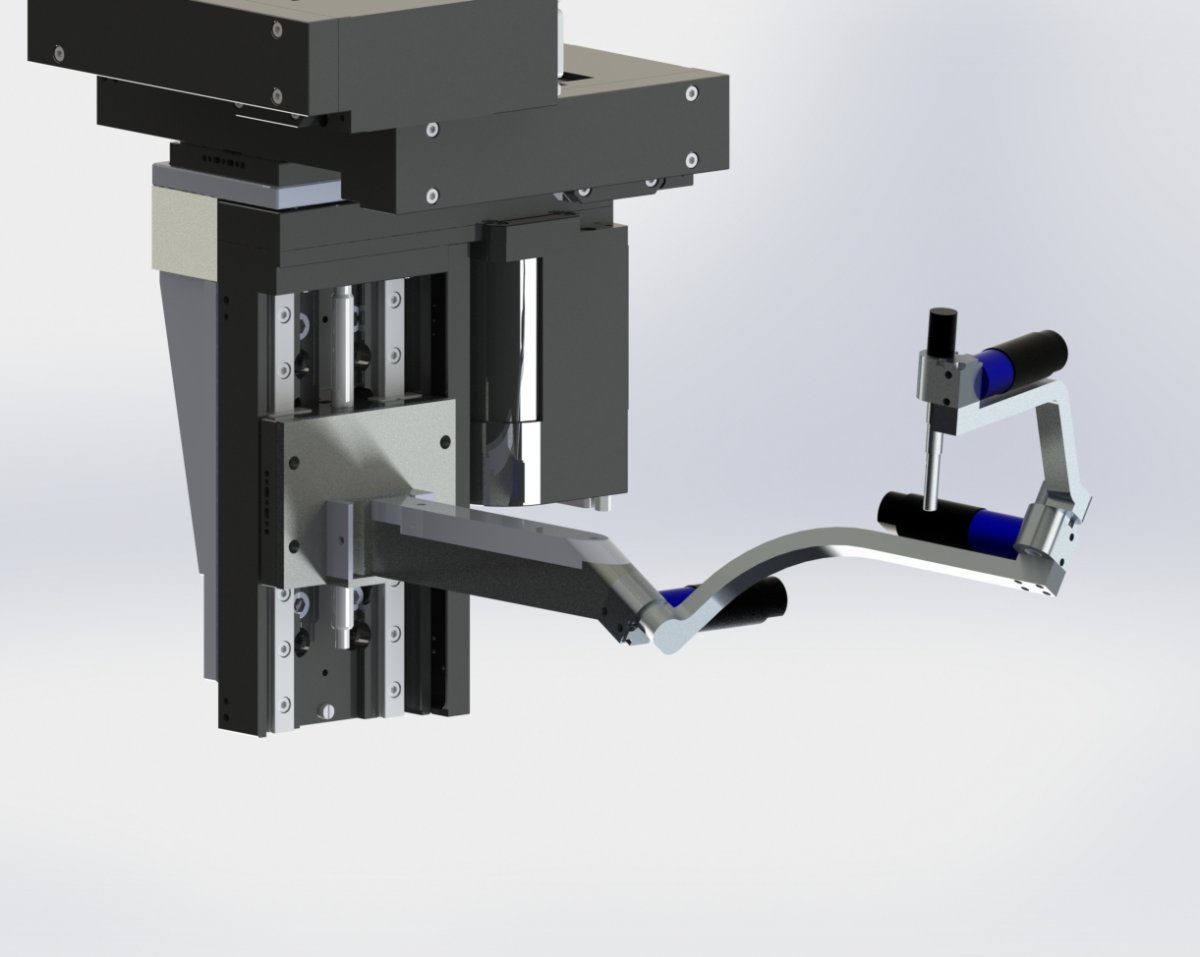
Realising this unmet surgical need has driven Professor Yann Nguyen to pioneer the development of a robotic system, designed to meet his specific needs. In collaboration with engineers from the Sorbonne University, Inserm, and Collin SAS, a French company specialising in devices and instruments for use in ENT, with additional funding from a private foundation for hearing (Fondation Pour l’Audition), RobOtol, was created.
First developed in 2009, this robot is suitable for use in otolaryngology surgical procedures such as stapedectomy, ossicular chain reconstruction, tympanoplasty, myringotomy and mastoidectomy. The system gained CE approval in 2016 and, since February 2018, Nguyen’s surgical team has used one of these robots on an almost continual daily basis.
Reducing collateral damage

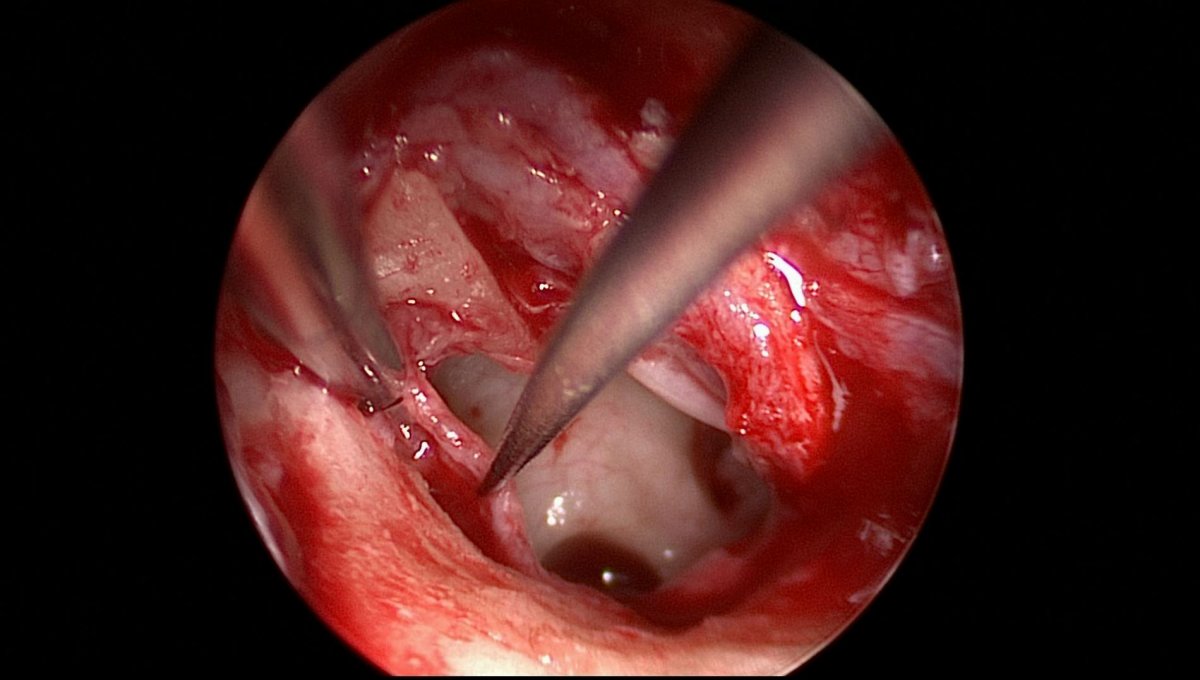
This July, for the first time globally, Nguyen used the RobOtol to insert the electrodes for a cochlear implant. Cochlear implantation itself is not new. First attempted more than four decades ago, it has been widely practiced for the past 25 years. The process involves replacing the role of the cochlea in hearing with an electrode array inserted into its immediate vicinity, which picks up electric currents from the conversion of sound waves directed by an externally placed microphone and processor. The auditory nerve is stimulated by these electric currents and transmits nerve impulses to the brain, where they are interpreted as acoustic sensations.
This microsurgery is normally carried out within a few hours as an out-patient procedure, under general anaesthetic. During the operation an electronic receiver (processor and antenna) is placed five mm under the skin and attached to the skull just behind the ear. An opening is created from the implant to the cochlea by drilling a three cm channel through the temporal bone to enable the passage of the device’s electrodes to the cochlea.
Ten patients from Berne in Switzerland have been operated on using a robot for this initial drilling phase, achieving accuracy that was unthinkable until now. However, for Nguyen this is not where a robot offers any advantage over a human in terms of outcome. For him, the part of the operation where the development of the RobOtol is so essential is so pass electrodes through the cochlea, which resembles a snail’s shell in structure, without causing unnecessary damage to the integrity and functions of this, even in profoundly deaf subjects, still vital organ.
No visual guidance
Additionally, the surgeon has no visual guidance at this stage because visibility is lost once the entrance of the cochlea has been passed and the trajectory of the electrodes is aided only by the surgeon’s touch. Nguyen stresses that this insertion of electrodes needs to be performed as slowly as possible to preserve the organ, and reduce inflammation, fibrosis and scarring to speed recovery and obtain the best possible outcomes.
His reasons for requiring this improvement are compelling. First, because the implant life is approximately 20 years, some patients, especially children, will need multiple procedures during their lifetime. Therefore, his aim is to inflict the minimal mechanical trauma possible with the first implantation, so as not to jeopardise the outcome of any second or even third future procedure. He also hopes that, in the longer term, solutions such as gene therapy and stem cell transplants will become a reality for restoring hearing among these patients, which is why he wants to retain the maximal integrity of the inner ear so that those he operates on today will not be excluded from future developments because of damage caused when they were younger.
Worldwide, two other RobOtols are in current use, one at the University Hospital of Liège in Belgium; the other in Shanghai, China. The fourth and most sophisticated machine is in the laboratory where it serves as a prototype to develop new procedures, such as this latest cochlear implant. The implants available today are all for manual use, but Nguyen is confident that, once more surgeons use the robot for this procedure, implant manufacturers will be keen to adapt their devices for robotic use.
Slow and steady
Using robot-assistance for a cochlear implant means that the electrodes can be placed at speeds as low as 0.1 sec/min with no tremor – something a surgeon would be unable to do. While adding a few seconds to the operating time, this slow advance of the electrodes is paramount to minimising trauma. Additionally, the robot can use more senses than a human in this environment. With no visual control, the surgeon is dependent on touch alone and, however good they are, their reactions to any impediment are slower by several milliseconds than a robot’s. With future improvements, the latter will be able to use heat sensitivity, measure hearing in real time and react instantly to any problem, thereby increasing the accuracy of procedures in a way no human can achieve.
According to Nguyen the RobOtol represents one of the first breakthroughs in cochlear implant surgery for 20 years. He considers that, until now, the technique had plateaued and was relying purely on the surgeon’s experience but now, thanks to these developments in robotic-assistance, the procedure has been forced into the 21st century and will remain state-of-the-art until an as yet un-invented technology supersedes it.
Profile:
Yann Nguyen MD PhD is Assistant Professor in the ENT Department, Otology Unit, Auditory Implants and Skull Base Surgery, at Pitié Salpêtrière Hospital, Paris. Prior to this, he was resident otorhinolaryngologist in the greater Paris public hospitals (AP-HP). In addition to his doctorate, he is a a specialist post-graduate in ENT, Head and Neck Imaging, Surgical Robotics and ENT, Head and Neck Cancerology. He has authored more than 50 papers, plus three patents and has won awards for pioneering work in robotics for ENT. Since September this year he has been promoting the use of robot-assisted surgery in inner and middle ear surgery via a club for current users and potential customers of the RobOtol system.
31.10.2019


