

Diagnostics
Iron deficiency and anaemia
Iron deficiency and resulting anaemia cause fatal comorbidities worldwide. Despite this, they are generally underestimated. Professor Lothar Thomas, specialist in laboratory medicine at Central Laboratory of the University Hospital of Frankfurt/Main, is calling for more information about the new laboratory parameters for diagnosis and monitoring of iron deficiency and iron substitution therapy.
The average prevalence of iron deficiency in Europe is five to 10 percent.* Whilst diagnosed in 4-8% of children between 13-15 years of age – at 20% – the highest prevalence is seen in women during their reproductive years. However, what no one ever says publicly is that iron deficiency also occurs often as a fatal comorbidity in chronic illnesses, such as kidney disease and renal insufficiency, chronic heart failure, intestinal diseases, obesity and tumours, as well as tumour treatment.
Why aren’t clinicians and public health groups more aware of iron deficiency and its seriousness?
Lothar Thomas: ‘One reason is that, despite its detailed knowledge and innovative laboratory diagnostics about iron deficiency and anaemia caused by iron deficiency, laboratory medicine has been unable to educate clinicians in a convincing way for the past decade. This partly has to do with the clinical acceptance of laboratory medicine, which varies significantly in Germany. In daily clinical routine, the laboratory is often seen as a service provider and less so as a competent, equal partner. Therefore, the laboratory is little consulted in the establishment and correction of disease-related clinical guidelines on diagnostics and therapy. Perhaps some of the innovative laboratory parameters or diagnostic algorithms are too complex to understand and interpret and therefore may be too complicated for the users. We must find new ways to convey our expertise and diagnostics in a practical way.’
Iron is generally a component of plant and animal food sources. The average daily need is only one or two mg, and the daily diet of central Europeans, with 15 mg to 20 mg, contains an excess of iron from food – so why are there iron deficiencies?
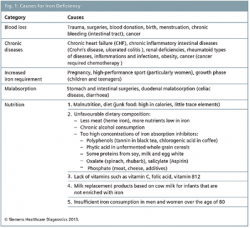
‘The causes for iron deficiency vary. First, it can be differentiated by events such as blood loss due to menstruation, blood donation, trauma, chronic inflammatory diseases and tumours. Secondly, there are situations with increased requirements, e.g. pregnancy, growth and high-performance sport and thirdly, the limited uptake through e.g. malnutrition, stomach, intestinal problems and inflammations.
'To illustrate this: menstruating women lose 50 mL to 60 mL of blood and therefore 25 mg to 30 mg of iron, which must be compensated. With 500 mL of blood loss, a blood donor has instantly 250 mg less iron. Usually, such an acute loss can be balanced by the stored iron of the body’s own reticuloendothelial system bound to ferritin (500 mg iron in women and 1,000 mg iron in men).
‘Subsequently, the iron storage must be quickly replenished.However, our body can only absorb a small portion of the need-dependent orally added iron. If we take 10 mg of dietary iron, up to six mg of it can be absorbed. However, we only absorb 15 mg of 100 mg of dietary iron, i.e. the absorbed quantity is less the more dietary iron is offered.’
Is there a difference between iron consumed in meat or plants?
‘It must be clearly stated that the heme iron from meat products – particularly “dark” meat – is significantly better absorbed than iron from food of plant origin. Women, who generally consume more vegetables and fruit than men, and particularly vegetarians are at a significant disadvantage. Only 10 percent of the iron content from plant sources is absorbed; so it’s not easy to balance any deficiencies with standard nutrition.
‘Therefore it can be concluded that iron requirement and iron supply are in an instable balance. After all, the German Society for Nutrition recommends men take 10 mg and women 15 mg of iron per day through their diet. However, in this context, it is important to have a sufficient quantity of vitamin C in the diet because enteral iron absorption is ascorbic acid dependent. Ingredients in coffee or tea immediately after a meal have a counterproductive effect.
When does iron deficiency become complicated?
‘Iron deficiency without anaemia is found three times more often than iron deficiency with anaemia. For as long as the iron deficiency has not developed into anaemia, we speak of an uncomplicated iron deficiency. However, it must always be understood as a precursor to anaemia. Problems arise, if the stored iron has already been depleted, or has not been adequately replaced or, in the event of increased requirements, the storage iron cannot be mobilised e.g. after stimulation with recombinant human erythropoietin (rHuEPO).
'We have this situation in inflammations with CRP levels of >5 mg/L. This is caused by the polypeptide hepcidin formed in the liver, which is the central regulator or iron homoeostasis. Under normal circumstances, an increase in this protein regulates the iron metabolism by slowing down iron absorption from the intestine, the iron transport to the placenta and the re-release of recycling iron from the reticuloendothelial system. On the other hand, if the iron requirement increases, the hepcidin level is regulated downward.
‘In chronic inflammations, the inflammation promoting interleukin-6 also leads to an increase in hepcidin level, which in the end leads to an anaemia caused by inflammation through this causes permanent blockade of iron release from the macrophages, which decompose old erythrocytes in the spleen. Serious iron deficiencies are then expressed as microcytic hypochromic anaemia. Therefore, it is important to recognise any iron deficiency in the early phase, prior to the development of anaemia.’
What are the signs and effects of iron deficiency?
‘There are many symptoms of iron deficiency. First, it should be determined when such symptoms occur. We differentiate between three stages: the storage iron deficiency (à iron supply), the iron deficient erythropoiesis (à iron requirement) and the iron deficiency anaemia. If the iron deposits are empty due to a negative iron balance, but the functional iron is not yet affected in its circulation, then there are no clinical symptoms of iron deficiency. If the iron deposits are depleted and less functional iron is now circulated, then it leads to an insufficient iron supply, the erythropoiesis.
‘The iron-dependent cell functions of the organisms (such as the iron-dependent enzyme of the respiratory chain) are just as affected. In this sub-clinical condition, we don’t see any anaemia; however, there can already be physical signs of discomfort. If the result is anaemia because the iron is not substituted, then the problems escalate. Often, patients only seek medical advice when they suffer severe discomfort, i.e. during the later progression of the sub-clinical and functional iron deficiency, or even after the iron deficiency anaemia has manifested itself. Patients feel tired and are running on a low “energetic flame”. Their quality of life is impaired. Particularly in children there is the risk of growth disorders due to severe chronic iron deficiency and neurological as well as cognitive losses can develop.These cannot be revised. Iron deficiency symptoms are expressed in many ways and it shows multiple symptoms.’
Part 2... To be continued in EH in 2015
* Source: The German Society for Haematology and Medical Oncology
18.12.2014








